
Changing The Way We Fight Covid-19
Israel was one of the few countries praised for its early coronavirus response and was heralded as an example to follow. But a reopening of the country has erased most of its early gains. Now the country braces for new restrictions and is under the threat of being in lockdown, as a second wave continues to spread.
How should the country move forward and can it continue to lead? Joseph Cox shares his thoughts on how Israel can best overcome the challenges of the pandemic in ways easily replicated by other countries as well...
------
There are two key coronavirus developments that should recalibrate Israel's approach to the virus:
1) A reduced death rate, relative to cases (see the chart below)
2) The massive death in developing nations due to economic disruption. There are almost twice as many people facing an acute hunger shortage suggesting about 19,000 people *a day* will die of hunger this year. This figure includes 6,000 children according to the World Food Program (WFP).
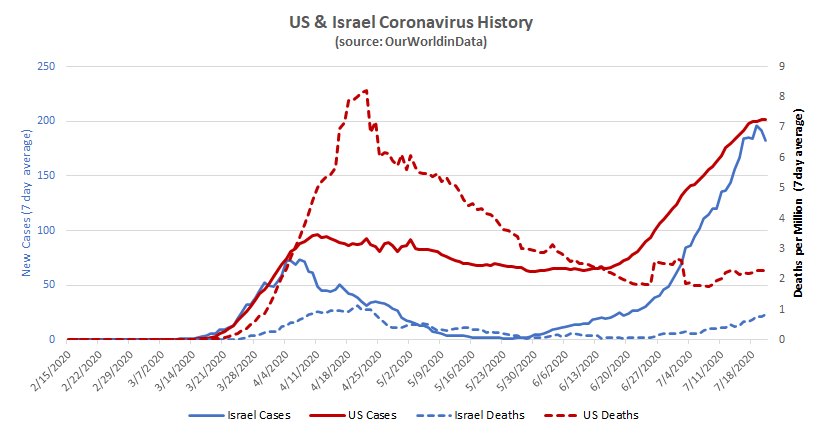
The moral response, I believe, is to open up the economy and aim for rolling resistance like the New York Haredi community has achieved. Of course, that community paid a terrible price - but death rates are far lower now than they were then (see the chart above). Other countries can follow the same model.
What policy change would I propose?
1) The evidence appears to be overwhelming: masks help. They might just blunt the viral load. So let's change the mask policy: every person caught without one in the vicinity of others is put into involuntary quarantine. That will be more effective than a fine we aren't collecting.
2) Allow all businesses to open and operate fully. We'll have more cases, but they'll be slowed by the masks. People might not choose to eat in a crowded restaurant, but we can allow the option.
3) Open the borders. After all, who are we kidding, there's no more risk from outsiders than insiders. Our economy needs travel and our aerospace industry is critical to our national strength.
4) Up the budgets for hospitals, temporary corona wards, hazard pay for nurses and doctors - hire people from less impacted countries. The economic boost will provide the funding for this.
5) Boost pensions to enable the old to stay as isolated as they choose.
6) Test nursing home staff/residents bi-weekly or when symptomatic. There are about 75,000 nursing home residents in Israel (from a Taub Study). Isolate cases in this population as fast as possible to minimize the most catastrophic spreads.
7) Keep 10-19 year old students in remote or pod learning (because they are great transmitters and don't need to be babysat) while opening schools for younger kids (who aren't good transmitters).
The Moral Choice?
6,000 additional children a day are dying of hunger in developing nations - and 13,000 others. The United States, Europe and Israel have lost 931 (mostly elderly) people a day, over the past 5 months. And that rate has fallen to 1,105 over the past month and 1,067 in the last week.
In terms of life-years lost, the distinction should be shocking. Studies have indicated the average person with corona lost 10 years - so 11,000 life-years lost a day in the West vs. 240,000 life years for the children alone - assuming they only had 40 years remaining in their own lives.
It is worse than that, of course. The lives lost in developing nations will continue until we reopen while the lives lost in the first world will only continue until we achieve some sort of imperfect herd immunity (either through widespread transmission as in NY or through a vaccine). We can save the lives of those in developing nations, now, by reopening. The longer we 'bump along' the more lives will be lost.
What about extra deaths?
With a reopening, death rates will rise. It took 22,000 deaths in a city of 8.4 million to get to where New York is now. But death rates have fallen by about 4/5ths per positive test in the US and they were always lower in Israel. Based on our first wave statistical sampling, Israel had a 0.14% mortality rate (vs. 1.4% in NYC). This would suggest somewhere around 2,000 additional deaths to achieve what NYC achieved with 22,000 deaths.
That is a terrible price to pay. But it is unclear that we aren't going to end up paying it anyway due to the limited length of individuals' immunity. If we 'bump along' people will be only occasionally exposed allowing continual reinfection due to extended delays between exposures. But if we allow faster transmission then people can have their immunity 'topped up' by more frequent exposures while they still have immunity. Individuals in NYC might not have long-lasting immunity, but the community seems to have 'rolling immunity.' I'm no epidemiologist so I'd welcome a critique of this idea.
To me the end result might be that through this policy of moderated exposure through masks we might actually save lives even in Israel.
What about morbidity?
This is the big challenge. The coronavirus causes significant damage in some significant portion of survivors. Some claim the figures are as high as 20%. I doubt that because it seems that fewer than 20% of cases are actually detected. In Israel statistical testing in early June suggested 250,000 cases in the 'first wave' but only 17,000 were detected by that point. There may be morbidity in the undetected cases but it is - so far- undetected.
Morbidity is a problem but so is a lack of nutrition in childhood. And, as with deaths, morbidity might be improved by 'topping up' immunity rather than long delays between exposures and thus more impactful disease.
Conclusion
I think Israel should be leading the Western world by making the moral decision that the lives of the world's poor matter too.
The world's poor don't need a hand out to reverse the catastrophe they face. The world's poor often survive - even if indirectly - on the manufacturing, mining, farming and migrant jobs provided by rich countries.
A culture of fear is killing the most vulnerable. In the West it is limiting economic life. In middle-tier economies like Egypt, it shows itself in the national hoarding of food.
We have something to fear other than fear itself. The virus is real and dangerous. But our fear, like an overactive immune response, is more dangerous than the cause of it.
We've taken 1.4 billion people out of extreme poverty in the last 30 years. Let's not lose all that we've gained.
Let's make the moral choice and get our economies open again.
----
Do you disagree? As I said above, I'm no expert. I could well be wrong. My goal is a conversation that goes beyond the virus itself.
Please think, share and even argue. We'll all be better for it.



@[Moon Kil Woong](user:5208), what's your take on the fight against #COVID19?
We should do everything we can, sadly we aren't and it shows. When a treatment that prevents Covid from being fatal comes around, which I believe we are on the cusp of, we can take these and other steps to enabling the economy to get back to normal. Until then exchanging life for business as unusual (it will not go back to normal no matter what social policy you take to stimulate the economy) is not a risk we or any nation should take.
The worse the disease gets in the country and the longer it lasts risks even worse economic effects will come into play as countries begin to take measures to prevent reinfection and business develops around you. If we don't do anything we are liable to get lumped into this pile of countries where you need to find a way to get what you need without them. This will undermine our country's economics and put us in a position where we fall behind the ROW economically.
I hadn't realized Israel had fallen so far from when it was touted as a leader in fighting COVID-19. They now rank as having the 6th highest death rate - right after the US! Shocking.
Some interesting thoughts. @[Judah David Powers](user:82828), you'd probably like this article.
Great article and some out of the box recommendations. Thanks for sharing!
Good article.
Infections are getting out of control in California. Not sure what we can do about it.
Test positivity rates and case counts in CA as well as deaths have been rising. But not anywhere close to that of AZ, FL or TX. For a state of its huge size, our deaths are lower than FL and TX on a recent daily basis, test positivity rates have been less than 1/2 those states and case counts on par with states 3/4 and 1/2 our size. CA’s size distorts some data. Yes, CA has a huge uptick but our hospitals are prepared and have room and our population are generally health guidelines followers and we’ve significantly rolled back reopening. With concerted efforts in mask wearing, hygiene and social distancing and effort to stop people from having private social gatherings like BBQs, we should be able to get things under control without another total lockdown... but it’s up to our population to act accordingly. We are much better positioned than TX, GA or Florida to do so without any lockdown.
Maybe you can totally shut down.
Of course, I don't think you could do it for long enough. I'd suggest draconian mask compliance to allow for moderated exposure. But, again, as I said in the article, I'm not an expert. My goal is to stimulate thoughtful conversation.
That's the problem though isn't it - shut down and cases drop. But the economy is destroyed, people's mental health suffers and some people even go hungry or can't afford rent. Open up and infections go back up and people die. We can't win. We need a vaccine.
As a stand alone, California could shut down for quite some time. That would limit deaths. Think about it this way: the state has huge resources many of which come from IT and entertainment - a lot of which can be perpetuated virtually.
So shut down, have self-driving cars (safe on streets without people or human drivers) deliver everything. Have very limited numbers of people packing stuff. You can limit human to human exposure for a few weeks and knock cases right down. Basically, send every person in the state food and suspend all rent and mortgage payments.
Then open up again, wait for cases to rise, and then do it again.
Rinse and repeat until vaccination rescues you.
The longer-term effects of this would be terrible. The economic malaise would have big impacts on mortality within the state - although they are far harder to measure. Some studies have suggested unemployment doubles mortality for the unemployed over the following two years - people like to live for a purpose. Then you have the effects on less rich places.
Finally you have the really broad question: At what point is saving lives worth taking away living? I wrote a dystopian short story on that one...
https://medium.com/me/stats/post/268cb891e075
A good read but his opinion is based on 2 highly irrelevant assumptions/statistics.
1. Haredi herd immunity in NY has led to decrease in death rate. This is false. The lower death rate is because of much lower virus prevalence, better testing, contact tracing and isolating of vulnerable populations and improved therapeutics. There is no evidence of herd immunity in any community on earth.
2. The false choice that any policy implemented in tiny Israel will have any effect on starving children in the developing world.
Given this person’s opinion is entirely based on these 2 unproven or irrelevant assumptions... this strategy recommendation is bunk. 😀
Actually, the entire world has been watching what every other country has been doing to see what works. Some small countries like South Korea, New Zealand, Iceland and even Israel (at least in the beginning) received a lot of attention because it seemed that they were winning the battle.
I had the same thought @[Jason Goldfischer](user:137878).
The haredi community was hit hard, with something like a 70% t0 90% infection rate. Then bam, no more infections. So I do believe they have achieved immunity. But immunity seems to only last about 2 months which makes herd immunity impractical - how to get everyone sick, fast enough, before the two months are up? And without overwhelming the hospitals?
@[Ayelet Wolf](user:10327), @[Jason Goldfischer](user:137878), Makes sense. But that's why the author mentioned "rolling resistance."
I mentioned rolling immunity because our immunity doesn't last more than a few months. A possible way to explain this community not regressing is that our immune system might stay primed for the disease due to some level of continued exposure. For me, masks remain important even if you *want* to encourage exposure. We know not all exposures are equal. If you get a big viral load it will hit far far harder. Virus will get through a mask, but probably not a blast of it which helps those who get infected. Masks, I believe, might well lead to far better outcomes even with infection. (Of course, as I said in the article, I'm not an expert - I'm just looking at the data.) The Haredi community is not the only interesting one. Take Sweden. They got hit hard (5% initial death rate vs. statistical infection rate vs 1.4% in NY and 0.14% in Israel because they basically didn't treat the over 70s or protect nursing homes). But they never really locked down. Nonetheless, their new case rate has fallen from 128 cases per million to 30? The people who had it three months ago don't seem to be getting it again. Their death rate has fallen from 10 per million to 1.5 - without lockdowns. The virus is still there, the positive test rate is still 3.5%. But new cases and deaths are falling nonetheless. For tests there can be all sorts of reasons (testing methodology being one). But for deaths we've got better treatment, weaker virus or increased immunity. This suggests some sort of increased immunity of either a healthcare or biological type.
"We know not all exposures are equal. If you get a big viral load it will hit far far harder." How do we know that? How does one send a "big" viral load vs. a small one? Can you please clarify? Do you mean like breathing on someone vs. coughing/spitting on them?
I used the wrong term in the comment. Higher viral load is how much you have, not how much you got hit with. As expected. high viral loads are bad... academic.oup.com/.../5865363
The right term is infection dose and it is a well-established concept.
Here's some tribal knowledge on this: www.latimes.com/.../masks-help-avoid-major-illness-coronavirus
I had a harder time finding formal papers. They tend to need to do animal studies to understand this better because it is hard to trace infection dose otherwise. Animals aren't exactly human, so there are very real limits. That said, here is a relevant study...
www.immunology.ox.ac.uk/.../dose-dependent-response-to-infection-with-sars-cov-2-in-the-ferret-model-evidence-of-protection-to-re-challenge
"Only high- and mid-dose animals developed mild multifocal bronchopneumonia alongside liver inflammation. "
In a way, I think this was first used with early innoculations. Before cowpox was discovered, they used to take pustules from those who had smallpox and insert them under the skin of the healthy. This brought on smallpox, but fatality rates were much lower as a result of the nature of exposure (not breathed in in a systemic exposure). It was a more limited exposure.
This all makes sense Joseph. Thanks for the explanation.
In terms of viral load I'd suggest spitting in their mouth or sneezing in their face would be very high. Having a few particles waft in from 20 feet away would be very low.
I can't believe Sweden fared so well. Are you telling me that @[DRM](user:130312) was right all along and the world never should have gone into lockdowns???
Yes, I've been right all along, Thanks. Joseph Cox, you can clearly see that no single country has been hit hard or faired poorly, if you open your eyes and look at the numbers. So, one more time. The worldwide death rate is currently 8/1,000ths of 1% or 640K. Which is approximately the same number of people who die from the flu, every year, year after year. But, the cost of the lockdowns around the world will not be fully measurable for months or years to come. Millions will die because of the lockdowns and/or live in poverty, because of the foolish actions of politicians around the country and around the world. If 10 times more people die from C-19 before this is over, it will still be less than 1/10th of 1 percent of the world population. No one can prove that the lockdowns did anything to reduce deaths. The lockdowns are Insanity!!!
Sweden has faired POORLY. They didn't isolate or protect the old and they got hit hard before there was much of any medical mitigation. Not as bad as mainstream Europeans, but far worse than other Scandanavians. Given that we know there are hereditary risk factors they didn't do well - just like the Haredi community in NY which got HAMMERED.
That said, despite all of that, rates are falling in Sweden and have collapsed in Ultra-Orthodox NY - suggesting that there is some sort of community immunity being estabished.
I'm not sure we can know how contagious kids are. Most will be asymptomatic (we know that much). But as a result, how many are being tested, and how much contact tracing is really being done? Kids are still a bit of a mystery here.
Newer reports indicate kids 0-9 are the least infectious group while those 10-19 are the most infections group (of any age). So school might be spreading but kindergarden is less likely to do so. Thus the suggestion that younger kids go to school but older ones do not.
The latest study in Israel indicates 67% were infected at home.
There really is no to very little evidence that kids under 10 transmit the virus. The argument that younger kids are not spreaders is based on the fact that there is little evidence to support kids as spreaders. There is no evidence because kids through 10 are the least likely to be studied, least likely to be tested and most likely to have been quarantined at home without many social interactions. So while there is no real evidence that kids under 10 spread the virus like adults, there also is no evidence they don’t. Here’s where common sense and basic virology comes in. There is no logical reason to believe that kids under 10 don’t spread the virus like a 12 or 20 year old. Like Mary said, viruses don’t have magic age cutoffs.
Reposting because it failed the first time...
This is the study - from the CDC website: wwwnc.cdc.gov/eid/article/26/10/20-1315_article
Methodology in a nutshell: "We analyzed reports for 59,073 contacts of 5,706 coronavirus disease (COVID-19) index patients reported in South Korea during January 20–March 27, 2020. Of 10,592 household contacts, 11.8% had COVID-19... We also found the highest COVID-19 rate for household contacts of school-aged children and the lowest for household contacts of children 0–9 years in the middle of school closure."
They have limits on the study, you can read them. But the statement still stands: "Newer reports indicate kids 0-9 are the least infectious group while those 10-19 are the most infections group (of any age)."
Note the word *indicate*. This is *not* "no real evidence". There is real evidence, it just isn't conclusive.
And, yes, there could be reasons for it. As far as I understand it, people transition from being biological children to being biological adults sometime between the ages of 10 and 19.
Yes, I’ve seen this study, there were not a lot of kids age 0-10 in the study and this comes back to virus prevalence. South Korea did not have huge numbers of cases or widespread community transmission. They had a well controlled and traced outbreak that likely didn’t give the virus time to penetrate the youngest and most isolated. We need to learn more before saying kids are not transmitters. We should not be making public health decisions based on one study from a country with universal masking, high compliance with rule following and a limited outbreak.
A lack of virus prevalence and widespread community transmission would actually make this study *stronger* in terms of measuring the impact of kids. You have a higher likelihood of isolating household contacts vs. community contacts.
Put another way: With community contacts clouding the data, age-based transmission effects would be very hard to measure. But if there are fewer chances of community infection then the likelihood of child contact being involved is *higher.*
I'd argue you couldn't do this study anyplace BUT where "there is universal masking, high compliance with rule following and a limited outbreak."
No study is perfect, no data is perfect, but that shouldn't stop us from learning or force us into paralysis from open-ended analysis.
Realistically, how can they even test for that? And is there some magical cut off, that on a child's 10th birthday he/she suddenly becomes infectious? I suspect a lot of these scientific studies are assumptions and guesses at best.
They trace to find those who were near them who tested positive earlier, I presume. Standard contact tracing. I'm sure the change is gradual. But I'm also sure it is weird. Perhaps the onset of puberty (adult in some respects but with far less risk aversion than 30-year-olds) provides the shift and it actually occurs a little older than 10 :)
I read a report that said most people are infected at home, presumably by their kids who were out and about at school/camp or with friends while parents are staying and working from home.
Like these articles that really make one think and reexamine our preconceived notions.
This is very eye opening. I've always thought of lockdowns as saving lives. I hadn't realized they could cost more to die from things like hunger, than the disease itself might have killed.
It is true that this realization as impacted by own thinking. But it's important to realize that we can't go back to the way life was before COVID-19. If we operated without any restrictions, and allowed the disease to spread unchecked, millions more would die.
Even with lockdowns and restrictions, we're getting closer to 1 million deaths every day.
Not from the virus. There have been fewer than 650,000 globally (https://www.worldometers.info/coronavirus/) from the beginning of the epidemic. There may well be undocumented deaths in the poorer parts of the world, but nowhere near 1 million a day.
Great article. I've seen others champion the concept of only locking up the elderly and at risk. But the elderly are the most susceptible to the disease and have been locked up for far too long already. Any many are dependent on others for help, as it is, making it hard to stay home. Both our mental and physical health will deteriorate further if we don't eradicate this disease soon. I'd rather keep everyone locked up for a shorter period and nip this thing in the bud once in for all.
One problem I've seen is that a lot of people assume "at risk" and "elderly are the same thing. But many others are at risk - smokers, asthmatics, expectant mothers, infants, diabetics, those who are overweight, the list goes on. It's far from just the elderly. When you add up all those people, it's quite a high percentage of the population.
Lots of people are at "higher" risk. It appears indo-Europeans are at far higher risk than east Asians. But an obese 30 year old is at lower risk than an otherwise healthy 70 year old.
Those who feel they are at particular risk can isolate themselves more. For example, they don't have to send their kids to school.
Where we can identify clear demographic classes with significant boosts in risk, we can enable isolation. Checks for the pregnant or those with medically diagnosed hypertension etc... But we should aim to limit the isolation somewhat so we can spread the virus well in less vulnerable areas.
(As an aside, I'm following this within the established rules. I'm mostly indo-European, my blood pressure is a bit high and my BMI is 27.5, I sent my youngest two kids to kindergarden this week despite significantly increased spread in my community. One got exposed to a special ed assistant and another diagnosed kid. I'm in isolation now but I do not regret the exposure and will not even if I get very sick. I am at slightly higher risk but my possibly exposure could actually limit risk for those at much higher risk and perhaps hasten the reopening of the economy. To paraphrase a poker player I know, you don't regret the hands you lose - you regret those you played wrong.)
Loading comments, please wait...