
TM Editors' note: This article discusses a penny stock and/or microcap. Such stocks are easily manipulated; do your own careful due diligence.

Image Source: Pixabay
Readers may be familiar with my writing on Galectin Therapeutics which I have discussed in detail for several years (on another financial website that I am favoring less and less compared to TalkMarkets). Those unfamiliar with Galectin Therapeutics (GALT), can reference my numerous previous articles.
As a quick summary for those unfamiliar with the company, Galectin Therapeutics is a clinical-stage biotech company developing galectin-3 inhibitors for the treatment of diseases. Their primary focus is on lead drug candidate, belapectin, for the treatment of metabolic dysfunction-associated steatohepatitis (MASH) cirrhosis, a late-stage liver disease with a very significant unmet medical need. Galectin-3 is known to drive inflammation and fibrosis in many different diseases, and it is also implicated in driving immune dysfunction and metastasis in many cancers. If belapectin can garner FDA approval, there is potential to open up the door for significant label expansion, similarly to how Abbvie’s (ABBV) pursued eight label expansions for Humira after its initial FDA approval.
The company recently released interim results of its phase 2b/3 MASH cirrhosis trial (NAVIGATE), which was designed to evaluate belapectin's safety and efficacy in treating MASH cirrhosis. Specifically, the goal was to prevent a key clinical outcome of cirrhosis decompensation: esophageal varices formation in patients with MASH cirrhosis. Because there is no approved drug for cirrhosis, and liver transplantation is the only curative option, peak sales of belapectin for the treatment of MASH cirrhosis in the United States are estimated to be $18 billion (according to a third-party analysis conducted by LifeSci).
The interim results of the NAVIGATE trial were released in late 2H 2024. Around that time, the company was subject to short-and-distort tactics that distorted investors’ perception of the company’s data release. These results were groundbreaking, unprecedented, and worthy of an FDA fast-tracked conditional approval, in my opinion. Because of the company’s recently generated clinical data, upcoming biomarker data, and benevolent shareholder-friendly financial support provided by billionaire Richard Uihlein, I believe the shares are undervalued and could be set up for a continued short squeeze as the shares have only just breached the levels they were at before the short-and-distort tactics began.
Galectin Therapeutics’ Largest Shareholders
One of the main reasons I don’t think shorts have a chance with Galectin is because of the company’s history of financial backing by Richard E. Uihlein, who serves as the Chairman of the Board of Directors at the company and who is founder and owner of the well-known distribution company, Uline. In addition to his leadership role, Uihlein has provided substantial financial support to the company through a series of credit facilities, convertible notes, and direct equity investments clearly demonstrating a long-term commitment that extends far beyond boardroom oversight. As such, he is Galectin’s largest shareholder. The Uihleins are also one of the top political donors in the United States as they contributed $59 million to campaigns and political causes in 2024, and over $250 million since 2016. Mr. Uihlein’s steadfast support of Galectin’s scientific mission has been both strategic and personal. If history is any guide, his continued presence and financial backing all but ensure that Galectin will remain well-capitalized and fully equipped to advance belapectin’s development for the foreseeable future.
Belapectin: The First Treatment with Clinical Endpoint Data for MASH Cirrhosis
The NAVIGATE trial, conducted by Galectin Therapeutics, evaluated belapectin, a galectin-3 inhibitor for its ability to prevent clinical progression in patients with compensated MASH (metabolic dysfunction-associated steatohepatitis) cirrhosis and portal hypertension, with a specific focus on the prevention of esophageal varices, a key clinical event in cirrhosis directly linked to mortality. Belepectin was designed to accomplish this by blocking the scarring process in the liver.
Belapectin’s Mechanism of Action
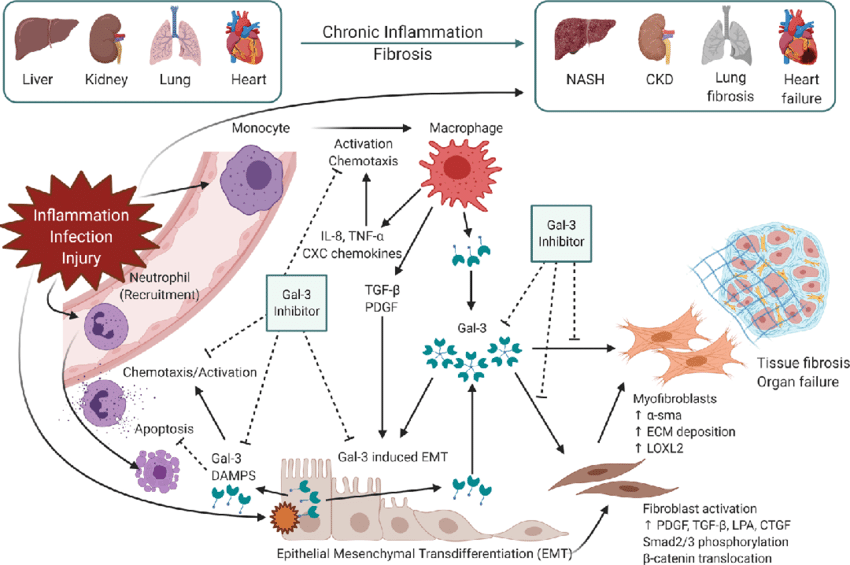
Belapectin is a complex carbohydrate-based drug that inhibits a protein called galectin-3. This protein is a carbohydrate binding lectin that drives fibrogenesis and amplifies inflammation across the body through several mechanisms, including activating macrophages, promoting myofibroblast proliferation, and sustaining extracellular matrix (ECM) deposition.
Galectin-3 levels are increased as a result of metabolic stress, hypoxia, and inflammation, and high galectin-3 levels are responsible for sustained fibrogenesis, amplified inflammation, and several mechanisms of immune dysfunction. Pathologically high galectin-3 levels and its effects on promoting inflammatory fibrotic diseases can be found across many different tissues, but is especially notable in hepatic, cardiac, renal, pulmonary, and dermal fibrosis, as well as in the stromal remodeling of certain solid tumors, and immune system dysfunction in the context of cancer.
The Therapeutic Potential of Galectin-3 Inhibition in Fibrotic Disease
Belapectin’s Clinical Significance
Belapectin is a first-in-class inhibitor of galectin-3. It is currently the only antifibrotic in development specifically for patients with compensated cirrhosis due to MASH (metabolic dysfunction-associated steatohepatitis, formerly known as NASH) who have portal hypertension but no esophageal varices. There are no FDA-approved therapies for this patient population.
Blocking galectin-3 at or before this stage of this fibrotic liver disease could stop or reverse disease progression, the clinical outcome of which is manifested in reduced complications of liver decompensation such as variceal development, variceal bleeding, liver failure, or the requirement for a transplant. But what are varices?
Similar to the etymology of varicose veins, esophageal varices are swollen veins that develop around the esophagus due to portal hypertension. Basically, when the liver scars, blood has a hard time traveling through the liver so it increasingly finds other paths to take, which causes the esophageal veins to swell. Eventually, the ballooned/swollen veins become enlarged to the point of becoming delicate and prone to bleeding. These ruptured veins that cause intense bleeding episodes are life-threatening, with high mortality during and after the event. Importantly as a measure for overall liver health, the presence of varices implies advancing liver fibrosis, progression of disease, and a worsening prognosis.

Esophageal Varices Infographic
The NAVIGATE Phase 2b/3 trial was designed to test whether belapectin can prevent the development of varices in this high-risk MASH cirrhosis population. This is a clinically meaningful endpoint because the appearance of varices signals decompensation, sharply worsening prognosis and increasing mortality risk.
Belapectin is a Potential Pipeline-in-a-Drug
Belapectin represents the leading clinical application of an antifibrotic through galectin-3 inhibition, currently focused on liver fibrosis due to MASH cirrhosis, though the therapeutic potential for belapectin extends far beyond hepatology.
Because fibrosis is a common outcome in multiple chronic diseases, and because galectin-3 drives fibrosis through the same (or a very similar mechanism) in many different tissues, belapectin could serve as a foundational antifibrotic drug in other fibrotic disease markets, targeting the fibrotic process at its molecular root rather than simply managing symptoms or inflammation.
Belapectin Stands Alone in F4 Cirrhosis: Competitive Playing Field is Weak
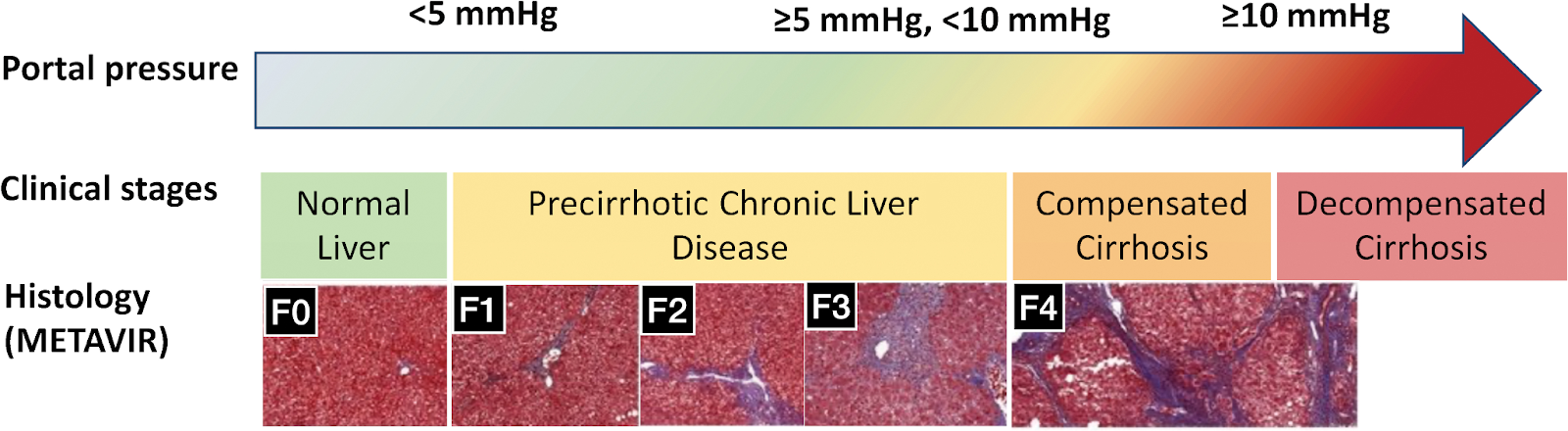
It is important to note that belapectin is the only direct antifibrotic in late stages of development in MASH, and is being tested in the later stage of F4 cirrhosis where the need and cost burden of MASH is greatest. Virtually all other drugs in mid-to-late stages of clinical development utilize primarily steatotic/metabolic mechanisms of action, where any effect (if any effect) on tissue scarring is indirect. These drugs being developed typically are being tested in F1-F3.
A steatotic drug is one that reduces steatosis, which refers to the abnormal accumulation of fat within liver cells (hepatocytes). Any antifibrotic effect or activity observed in F1-F4, using MASH drugs with a steatotic mechanism of action, is a secondary consequence of reducing the lipid burden. The belief is that multiple combinations of drugs will be needed and the only current option, Madrigal’s (MDGL) remetirom, makes it clear that there is significant room for improvement.
It is also understood that in F4/cirrhosis, disease progression is driven by inflammation, hypoxia, and fibrogenesis, so safe steatotic drugs might be minimally helpful, but direct antifibrotics are expected to be the most useful single agents.
Resmetirom Criticism
In a recent 2025 Hepatology letter, Sherker and Hoofnagle offer a pointed critique of Madrigal’s resmetirom (Rezdiffra), highlighting its relatively modest efficacy and high cost compared to other MASH therapies. Importantly, Dr. Sherker (hepatologist and Program Director at NIDDK) and Dr. Hoofnagle (Director of Liver Disease Research at the NIH) are considered key opinion leaders in the space.
They note that resmetirom achieved MASH resolution in only 26% of patients and fibrosis improvement in 24%, at a steep monthly cost of $3,500. In contrast, vitamin E, costing just $10/month, showed 43% MASH resolution and 19% fibrosis improvement, while semaglutide and tirzepatide (the extremely popular GLP-1 agonist weight loss drugs) demonstrated substantially superior results at 59% and 62% MASH resolution, and 43% and 51% fibrosis improvement, respectively at significantly lower costs ($1,200–$1,500/month).
|
Agent |
Rate of resolution of MASH (%) |
Rate of improvement of fibrosis (%) |
Monthly cost* |
|
Resmetirom |
26–29 |
24–26 |
$3940 |
|
Vitamin E |
36 |
41 |
~$15 |
|
Pioglitazone |
47 |
44 |
$4 |
|
Semaglutide |
36–59 |
32–49 |
$1349 |
|
Tirzepatide |
44–62 |
51–55 |
$1060 |
*Monthly cost estimates from relevant issues of The Medical Letter.
**Generic.
Adapted from Journal of Hepatology
The letter emphasizes that, despite FDA approval based on surrogate histological endpoints, resmetirom lacks evidence for preventing cirrhosis progression, decompensation, or liver-related mortality. Furthermore, it has not been adequately studied in true F4 cirrhosis (stratifying patients properly and with low platelet counts), where the clinical need is greatest. These points, coupled with the drug’s premium pricing and limited real-world data, make the letter a damning indictment of resmetirom’s current positioning, urging caution and demanding proof of meaningful long-term clinical outcomes. Furthermore, a recent Hepatology article examined real-world usage of resmetirom in MASH patients with F2-F3 fibrosis, which revealed a terrible adverse effect profile with 13% of patients discontinuing treatment due to adverse events. As these adverse events typically are amplified in cirrhosis, the resmetirom tolerability profile doesn’t bode particularly well for Madrigal’s MASH cirrhosis aspirations.
Efruxifermin Concerns
Similarly to resmetirom’s issues, there are concerns regarding the scientific rigor and reliability of Akero Therapeutics’ (AKRO) inclusion of F4 cirrhotic patients in its clinical trials for efruxifermin, due to its reliance on biopsy-confirmed fibrosis staging. Inherent and reader-specific biopsy variability exists when biopsy-staging liver slides, particularly at the F4 borderline zone. This raises concerns about the inconsistent classification of compensated cirrhosis. Relying heavily on histology to define cirrhosis and guide inclusion or exclusion in clinical trials without using other metrics may lack sufficient specificity to consistently differentiate F4 patients from advanced F3 populations.
There are also theoretical safety concerns with efruxifermin because it is an analog of fibroblast growth factor 21 (FGF21), which is an endogenous hormone. FGF21 has a range of actions, influencing mitochondrial energy flux, insulin signaling, and modulation of the neuroendocrine axis. Chronic (or supraphysiologic) FGF21 signaling, which is possible with efruxifermin’s long half-life, could disrupt homeostasis and increase oncogenic (including perhaps hepatocellular carcinoma, a complication of cirrhosis) and endocrine risks that are under-detected in short-term clinical trials.
Preclinical studies have implicated continuous FGF21 overexpression in bone mineral density reduction and hypothalamic-pituitary axis interference. The safety and tolerability outcomes associated with chronic FGF21 overexpression may be inadequately examined in Akero’s currently generated and published data so far. Therefore, the long-term tolerability of efruxifermin in cirrhotic MASH patients, especially those with reduced bone density, impaired hepatic function, or disrupted endocrine systems, remains questionable.
Imprecise F4 inclusion criteria and mechanistic uncertainty around long-term FGF21 safety and tolerability should increase investors’ doubts regarding the reproducibility, generalizability, and extrapolation of efruxifermin’s currently published efficacy and safety profile. Long-term studies with stricter enrollment criteria, endocrinologic monitoring, and additional long-term safety data are essential to de-risk its application for cirrhosis patients.
Galectin’s Clinical Trial Results
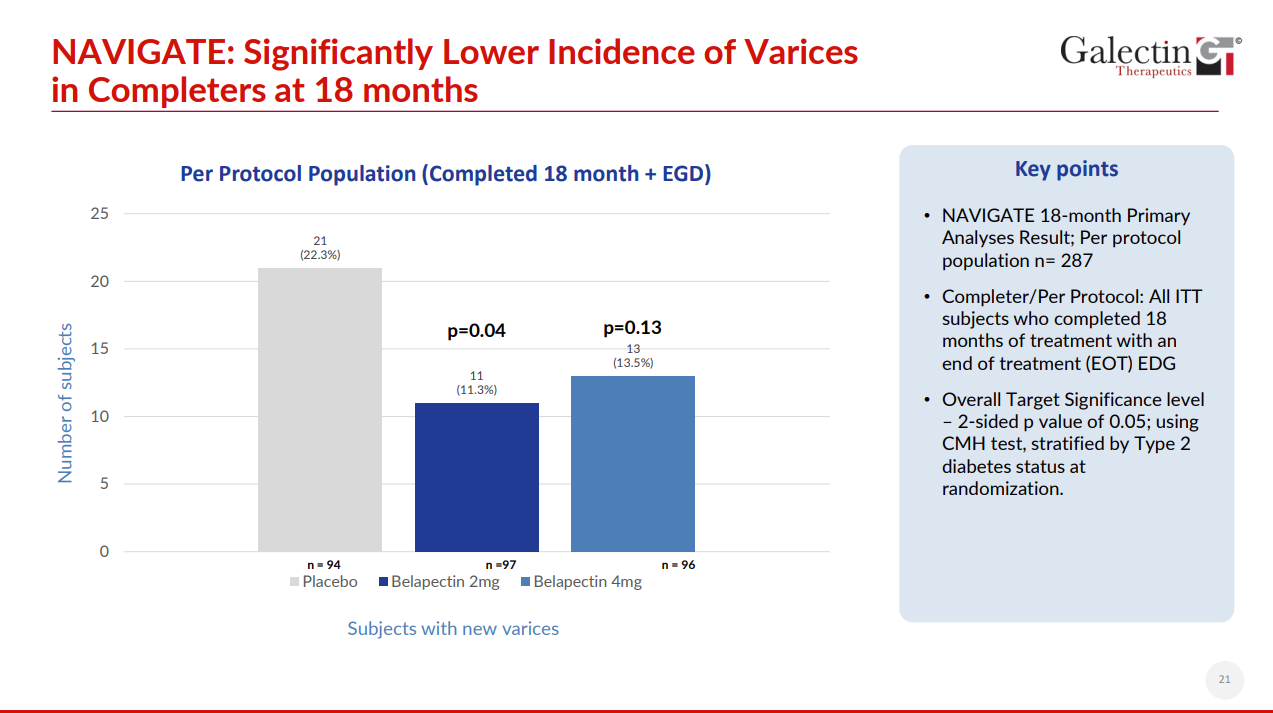
The results of the Navigate trial in true F4 cirrhotics with a clinical endpoint were nothing short of groundbreaking in a condition with no approved therapeutic. The trial did not meet its primary endpoint in the intent-to-treat (ITT) population because a large portion of patients did not show up (during the COVID pandemic) to their follow-up EGDs. However, Belapectin did demonstrate statistically significant reductions in esophageal varices development for patients who actually completed the study per protocol (and who showed up at the end of the study to see if they had varices development), particularly at the 2 mg/kg dose. Thus, the NAVIGATE trial repeated and validated the most clinically significant and promising signal from the NASH-CX trial: that belapectin, by inhibiting galectin-3, can reduce the formation of esophageal varices in patients with MASH cirrhosis. This is a direct replication of a pre-specified subgroup finding and was prospectively tested, statistically significant, biologically plausible, and consistent in dosage and patient selection.
Although the primary analysis based on the ITT population did not achieve statistical significance, this result was heavily confounded by the COVID-19 pandemic, which led to over 70 patients (nearly 20% of those enrolled) missing their required endoscopic assessments (esophagogastroduodenoscopy, a.k.a. EGDs), the core diagnostic tool for detecting new varices. These missing data undermined the reliability of the ITT analysis.
However, in the per-protocol population which only included patients who completed all study procedures (including EGD s) on belapectin at 2 mg/kg demonstrated a 49.3% reduction in new varices formation compared to placebo (p = 0.04). Importantly for potential FDA approval, the magnitude of efficacy was more pronounced in the U.S. subpopulation, where a 68.1% reduction was observed (p = 0.02). These findings are consistent with and confirm the antifibrotic and variceal prevention signal previously seen in the Ph2 NASH-CX trial. If belapectin was used to treat patients in somewhat earlier stages of cirrhosis or liver fibrosis, it is very possible that varices would be almost completely prevented.
Galectin Therapeutics Corporate Presentation (May 2025)
The reduction in variceal formation is aligned with positive signals from non-invasive tests (NITs). Namely, liver stiffness ultrasound measurements using FibroScan showed were improved in patients treated with belapectin. With belapectin 2mg/kg, patients experienced liver stiffness measurement (LSM) reductions of −3.48 kPa, −4.60 kPa, and −2.72 kPa at weeks 26, 52, and 78, respectively, while placebo patients showed no change. LSM reductions and prevention of variceal formation together represent congruent findings that support the drug’s mechanism as a true antifibrotic.
Belapectin also generated an excellent safety and tolerability profile, with no serious drug-related adverse events, a critical consideration in cirrhotic patients who are extremely vulnerable to drug toxicity.
From a regulatory standpoint, the NAVIGATE trial supports a compelling case for conditional (accelerated) approval. This is supported by a favorable risk-reward profile, with no known, observed, or mechanistically theorized risk for the patient. The case is strengthened by addressing a highly unmet medical need where patients eventually need a liver transplant, of which there are only ~10,000/yr to serve an estimated 3.3 million MASH cirrhosis patients in the United States. In other words, many of these people will die if untreated, and so given belapectin’s efficacy and benign safety profile, it could be considered unethical for the FDA not to grant conditional approval.
More technically, belapectin addresses a major unmet need in a population with no approved therapies, demonstrates a replicated clinical benefit in delaying variceal development, and shows supportive biomarker evidence of fibrosis reversal. The drug has also received Fast Track designation from the FDA and with the consistent therapeutic effect demonstrated across two independent trials, belapectin is strategically positioned for a potential conditional approval with probable phase 3 confirmatory trials.
Real Clinical Outcomes
Belapectin is currently the only drug in development for MASH that has demonstrated clinical outcome, i.e. a statistically significant reduction in the development of esophageal varices in a small phase 2 clinical trial and a larger pivotal trial. As variceal development and eventual variceal bleeding are important decompensating events in cirrhosis, these outcomes represent real tangible outcomes for patients that can drastically affect their well-being.
As the only drug to demonstrate such outcomes, belapectin is set apart from other commercial and late-stage developmental therapies like Madrigal’s conditionally approved resmetirom and Akero’s efruxifermin. Clinical trials testing these compounds have only reported histological (biopsy) or other surrogate endpoints, rather than cold hard clinical outcomes, which are the highest level, most robust indicators of patients’ health.
MASH Regulatory Landscape is Changing
The FDA’s messaging to Madrigal Pharmaceuticals even after granting accelerated approval for resmetirom based on biopsy-driven histological improvements in NASH and fibrosis has been unambiguous: further approval and potential label expansion, particularly into cirrhotic populations, will require demonstration of clinical benefit, not just tissue-level changes. This is because biopsy-based assessments, while historically useful in NASH trials, are deeply flawed as endpoints when used alone, particularly in advanced disease stages.
There are several reasons why liver biopsy, though once considered the “gold standard,” is increasingly viewed as insufficient and even misleading:
1) Biopsies are subject to sampling variability as liver fibrosis and other histological features of MASH are not evenly distributed. A biopsy samples ~1/50,000 of the total liver volume, making sampling variability a likely factor.
2) Even among expert pathologists, observer reading variability is very significant, where pathologists can very often disagree on how to score a slide.
3) Less important to data integrity, but more practically, liver biopsy is invasive and carries risks of causing bleeding and pain. Thus it is impractical for repeated or routine assessment, especially in fragile cirrhotic patients where they are at a low risk of death just from liver biopsy.
4) Related to expert observer unreliability, biopsy slide scoring systems are subjective and not purely quantitative.
Due to these limitations and drawbacks, the FDA and the MASH industry have increasingly emphasized the need for noninvasive endpoints in earlier stages of MASH, as well as clinically meaningful outcomes like delayed progression to cirrhosis, prevention of varices of variceal bleeding, and reduction in other hepatic decompensation events.
Belapectin is the first and only drug to demonstrate such a clinical outcome in compensated MASH cirrhosis as it showed a significant reduction in new variceal development in two independent trials (NASH-CX and NAVIGATE). To reiterate, this is not a surrogate or a biomarker, it is a direct clinical manifestation of disease progression, one with clear prognostic and regulatory weight, and clinical relevance to a patient and their doctor.
In contrast, while resmetirom has shown histologic improvements such as resolution of steatohepatitis and some fibrosis regression it has not yet demonstrated an impact on clinical events like portal hypertension, varices, or decompensation. The FDA's requirement for an outcomes trial and future demand for real clinical event data in cirrhotic cohorts reflect this regulatory shift. Similarly, efruxifermin’s early fibrosis regression data, while encouraging, remains preliminary and limited to surrogate endpoints, with no clinical outcome data and incomplete stiffness metrics.
Regulatory Shift at FDA Puts Galectin in the Catbird Seat
Galectin Therapeutics’ belapectin stands alone in its demonstration of a real, replicable clinical benefit in a patient population with no approved therapies. Placing it in a unique regulatory and therapeutic position. Its success in preventing varices, coupled with credible liver stiffness reductions without placebo anomalies, gives it an edge not only scientifically but also in the eyes of regulators. As the FDA moves decisively away from relying solely on flawed biopsy endpoints, a move supported by industry KOL opinions, Belapectin’s evidence base aligns squarely with what the agency is now demanding: proof that a drug changes the course of disease in a way that matters to patients—not just under a microscope on a histology slide.
In the race to develop effective antifibrotic therapies for advanced liver disease, belapectin (Galectin Therapeutics), resmetirom (Madrigal Pharmaceuticals), and efruxifermin (Akero Therapeutics) have emerged as leading candidates after the fall of Intercept Pharma which I called for when it was still the darling of the MASH treatment companies. While each of these therapies is promising for a unique mechanism of action and leading positions within each class of drug (galectin-3 antagonists, THRβ agonists, FGF21 analogs), stark differences emerge when examining reliability of clinical data, mechanisms of action and their respective safety profiles, and studied target markets.
Strength and Reliability of Belapectin’s Clinical Data
Of the three leading therapies in development for MASH-related cirrhosis, belapectin stands alone as the only agent to demonstrate both a statistically robust reduction in liver stiffness and clinically meaningful prevention of cirrhotic progression in a well-characterized, biopsy-confirmed, high ris F4 patient population. This MASH population experiences the highest burden to the healthcare system and represents the most unmet clinical need, while being the MASH population with the least amount of near-term direct competition. What sets belapectin apart is not only its efficacy but the reliability of its clinical signal, which emerges from a rigorously defined population of patients with established, uncompensated cirrhosis where placebo effects are expected to be virtually nonexistent if the trial enrollment filters are applied correctly.
In earlier-stage MASH trials (F1–F3), observed placebo response rates are typically in the 10-20% range and are often driven by spontaneous or unprompted regression. These placebo responses could be attributable to several factors including lifestyle changes or histologic misclassification at baseline or end-of-study.
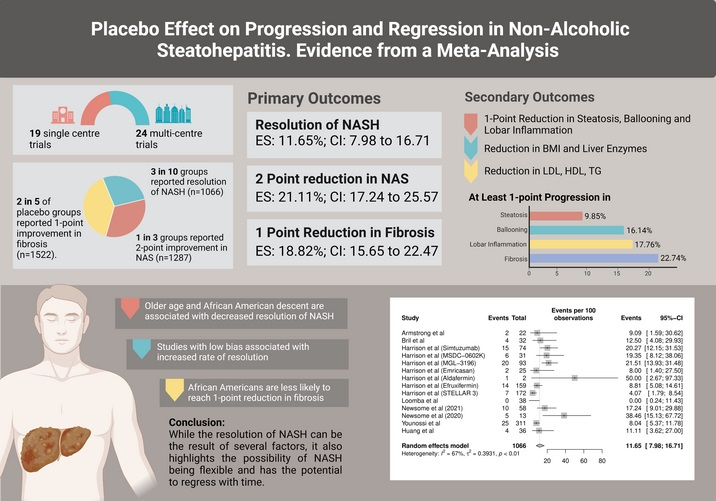
Placebo effect on progression and regression in NASH: Evidence from a meta‐analysis. Hepatology.
In contrast, patients with well-defined cirrhosis (F4), a structurally advanced and biologically entrenched condition where the extracellular matrix is considered almost permanently remodeled, generally do not undergo spontaneous regression of MASH stage. Cirrhosis is characterized by regenerative nodules and what is at least currently considered irreversibly distorted liver architecture. Thus, unprompted regression of cirrhosis in placebo-treated patients theoretically should be—and is clinically observed to be—exceptionally rare. This concept has been observed as true when stringent enrollment criteria and non-invasive confirmation tools (e.g., elastography, FibroScan, ELF score) are used to eliminate borderline or misclassified “late-F3” patients in clinical trials.
Case in point, Belapectin’s trial design in the NAVIGATE study incorporated strong screening criteria to ensure that the enrolled population exhibited true advanced cirrhosis and no misclassified, borderline F3 cases. This methodological rigor enhances confidence that observed clinical outcomes like the primary endpoint, the formation of new varices, are only attributable to the therapeutic agent, not statistical noise or spontaneous regression from misclassified F3 patients. Indeed, the placebo patients in the NAVIGATE trial experienced no discernable or meaningful change in LSM.
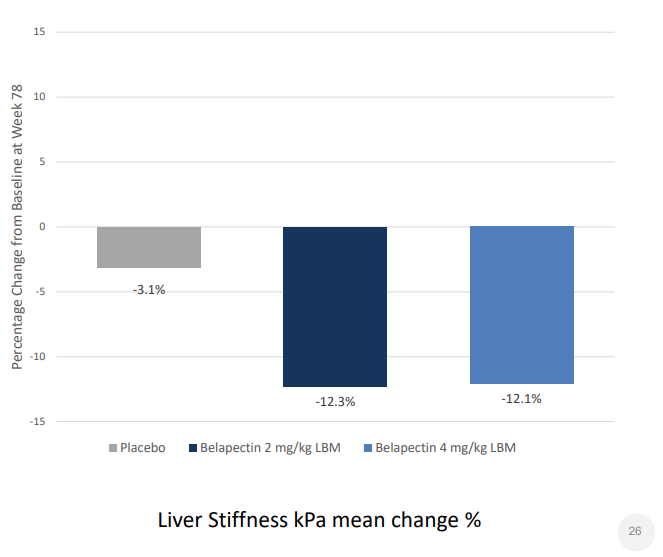
Change in LSM in NAVIGATE Trial: Placebo vs. Belapectin 2mg/kg, Belapectin 4mg/kg
Weakness in Efruxifermin and Resmetirom Cirrhosis Data Reliability
Efruxifermin and resmetirom have shown promising efficacy signals in earlier-stage, noncirrhotic MASH populations. However, in their cirrhosis endeavors, Akero and Madrigal appear to have failed in enrolling a pure patient population of compensated cirrhosis F4 patients. This is evidenced by their generation of “cirrhosis” efficacy data with placebo response rates that are biologically and practically implausible for true cirrhotics, calling into question the integrity of trial enrollment criteria and stratification. Data integrity issues are not an unfamiliar issue with Akero. Last year, a class action lawsuit was filed against Akero, following their SYMMETRY study, citing data integrity issues with enrollment criteria and a subsequent decision to exclude patients from topline analysis. While efruxifermin and resmetirom remain promising, the impaired data integrity and evidence of placebo responses in cirrhosis patients introduce ambiguity into the treatment effect size and also raise concerns about whether the therapeutic impact can be reliably reproduced in a true F4 patient population.
Belapectin’s LSM Data Supports Evidence of Clinical Outcomes - With No Placebo Effect
Belapectin’s efficacy is clear given the credibility of its clinical context, including an enrolled patient population where placebo responses approach zero, and where any signal of disease stabilization or reversal carries far greater meaning. As a drug with a direct antifibrotic mechanism that is clinically validated (in two studies—NASH-CX and NAVIGATE) this positions it uniquely among MASH candidates with cirrhosis indications.
Belapectin’s data from the NAVIGATE trial are compelling. In patients with compensated MASH cirrhosis (F4) and portal hypertension, belapectin at 2 mg/kg produced a mean liver stiffness reduction of −4.60 kPa at Week 52 (p < 0.0001), sustained at −2.72 kPa by Week 78. But perhaps more important than the absolute reduction is the credibility of the comparison: the placebo arm in NAVIGATE showed no meaningful improvement, a critical distinction. This is the only major antifibrotic trial in an F4 population where the placebo group demonstrated the expected natural history of worsening or stable liver stiffness rather than an unexplained placebo-driven improvement.
Comparing Galectin’s Cirrhosis Data to Madrigal’s and Akero’s Data
In contrast, both Madrigal and Akero report liver stiffness reductions in their placebo arms, casting significant doubt on the true magnitude of the treatment effects they claim, and the patient population that they enrolled in their cirrhosis trials. Any antifibrotic trial showing improvements in liver stiffness among placebo recipients must be scrutinized carefully, as such results defy the expected progression of cirrhosis and undermine the biological credibility of the drug-placebo differential as well as the clinically understood natural history of untreated disease progression.
Belapectin not only shows a credible, placebo-controlled reduction in liver stiffness but also demonstrates extraordinary protection against clinical worsening. In NAVIGATE, only 11.7% of belapectin-treated patients experienced >30% worsening in LSM versus 23.9% in placebo. For patients with >10 kPa worsening, the reduction was even stronger: 4.3% with belapectin versus 12.5% in the placebo group. When combining both severe worsening criteria (patients experiencing both >10 kPa and >30% worsening) to refine the efficacy signal and reduce noise, 4.3% of belapectin patients progressed compared to 11.4% of placebo. These figures reflect a halt in the progression towards irreversible cirrhotic decompensation.
By contrast, Madrigal’s Resmetirom, though reporting a greater absolute liver stiffness reduction of −6.7 kPa over two years, did so in a broader, less-defined population, and critically, did not isolate F4 patients in its analysis. Furthermore, the presence of a liver stiffness reduction in the placebo group casts doubt on the net drug effect, raising questions about the reliability and interpretability of the signal. Similarly, Akero’s efruxifermin reported impressive rates of one-stage fibrosis improvement (22–24% within 36 weeks) but failed to provide direct liver stiffness (kPa) data and did not isolate F4-specific outcomes. Akero’s placebo arm also showed response-like effects, diminishing confidence in the treatment delta. In the absence of credible placebo-controlled liver stiffness data and defined F4 performance, claims of antifibrotic superiority from Madrigal and Akero become speculative at best.
In summary, belapectin offers the most clinically validated and biologically credible antifibrotic data profile among current late-stage candidates for MASH cirrhosis. Unlike its competitors, it has demonstrated a statistically significant liver stiffness reduction with a replicated, stasitically significant clinical outcome: preventing the development of esophageal varices. These results are grounded in a trial where the placebo group behaved as expected a rarity in NASH/MASH drug development and a major validator of belapectin’s effect. Comparatively, the data from resmetirom (Madrigal) and efruxifermin (Akero) should be interpreted with caution, given the improvements in their placebo groups, which are paradoxical and unexplained if these patients are assumed to be true F4 cirrhosis patients. Therefore, while Madrigal and Akero’s drugs are promising in earlier stages of MASH, the totality of evidence places belapectin at the forefront of antifibrotic development for advanced cirrhosis, with a uniquely credible efficacy and safety profile deserving of regulatory priority.
Future Potential for Ubiquitous Antifibrotic Mechanism of Action Drug
Belapectin’s therapeutic potential as a galectin-3 inhibitor extends far beyond hepatology. Since fibrosis is not a liver-specific process; it is a pathological reparative response to chronic injury in various tissues, with biomolecular commonalities spanning diverse tissues, including galectin-3’s role in fibrogenesis including but not limited to acting on fibroblasts and myofibroblasts’ TGF-b receptors and integrins to amplify and sustain fibrogenesis, acting as a chemoattractant and inflammatory mediator for macrophages, and cross-linking cell-cell and cell-ECM interactions via oligomerization.
As such, there is a host of research that has been and continues to be conducted on galectin-3 on galectin-3 inhibition for other fibrotic (and oncologic) disease indications including but not limited to:
- Cardiac fibrosis (heart failure/cardiomyopathy) and arrythmias: galectin-3 drives myocardial fibrosis, contributing to ventricular wall stiffening, reduced diastolic function, tissue remodeling that contributes to impaired electrical signaling. Elevated serum galectin-3 has been shown to be a negative prognostic for these diseases, and preclinical models inhibiting gal-3 in cardiac disease show promise.
- Idiopathic pulmonary fibrosis (IPF): Interstitial lung fibrosis is driven by alveolar macrophage and fibroblast-produced gal-3, which drives ECM production just like in the liver. In preclinical models, galectin-3 inhibition has shown promise in treating lung fibrosis (and in treating portal arterial hypertension—PAH).
- Cancer (tumor fibrosis and immunosuppression): gal-3 contributes to building an immunosuppressive and stroma-protected local tumor environment by activating cancer-associated fibroblasts (CAFs), promoting angiogenesis, and suppressing anti-tumor immune responses via a range of pathways including causing T-cell exhaustion. Tumor ECM (stroma) promotes tumor growth and metastasis but also impairs drug penetration and physically blocks immune cell infiltration. As such, belapectin has been shown to synergize with Merck’s (MRK) Keytruda, the best selling drug in the world. This preclinical and clinica data Galectin and its research collaborators generated suggest that galectin-3 inhibition may re-sensitize tumors to checkpoint inhibitors by alleviating T-cell suppression. However, there is frankly a long list of postulated mechanisms by which inhibiting galectin-3 may aid in cancer treatment, particularly in immunotherapy combination treatment, which I previously wrote about in a blog post.
- Kidney and pancreatic fibrosis: galectin-3 is also thought to drive chronic kidney disease, diabetic nephropathy, chronic pancreatitis, fibrotic complications of type 2 diabetes. Notably, evidence suggests gal-3 interferes with the insulin receptor, contributing to insulin resistance (not just fibrosis)
Galectin Therapeutics does not appear to currently have the capabilities to test belapectin in all of these areas, but its possible that the label expansion potential for belapectin could help attract a major pharma as an acquirer or licensee. This kind of blue-ocean potential is certainly attractive, given belepaectin’s antifibrotic mechanism of action, which is more or less the same across a wide range of organs and tissues, is also set to be verified with advanced biomarkers measuring fibrosis in real-time.
Advanced Biomarkers for MASH Will Disrupt Everything
Dynamic biomarkers like PRO-C3, PRO-C6, and CTX-III (also known as CTX111) are gaining traction in the MASH field as blood-based nonbiopsy liver fibrosis diagnostics. These collagen-related biomarkers reflect the real-time construction and breakdown of the ECM and therefore provide insight into whether a patient's disease is actively progressing or regressing. This dynamic measurement may be useful in MASH in general, but particularly essential in cirrhosis specifically, where conventional tools of the last decade such as liver biopsy or LSM are not effective at capturing fibrogenic or fibrolytic momentum. Think of FibroScan as a function or value, and the fibrogenesis/fibrolysis balance measured by these advanced biomarkers as the function’s derivative, indicating what direction FibroScan will go in the future.
Among these, PRO-C3 has emerged as a leading marker of ongoing fibrogenesis, specifically reflecting the formation of type III collagen—a major component of newly deposited scar tissue in response to chronic liver injury. In the NAVIGATE trial of belapectin, blood samples were collected every six months, allowing for serial quantification of PRO-C3 levels. Unlike a single binary clinical endpoint like esophageal varices (assessed via EGD at Month 18, where over 70 patients missed their procedure due to COVID), these longitudinal biomarker data are continuous and time-resolved, meaning they remain available even when EGD endpoints are missing. This offers a significant correction to the Intent-to-Treat (ITT) limitations of the NAVIGATE trial. By capturing a biochemical fingerprint of disease activity at regular intervals, PRO-C3 and related biomarkers can reveal therapeutic effects even in patients who were lost to clinical endpoint assessments helping to preserve trial power and interpretability.
But PRO-C3 alone does not tell the full story. It captures fibrogenesis, but not fibrolysis. CTX-III (collagen type III degradation) is a measurement of breakdown and remodeling of scar tissue. Lastly, PRO-C6, derived from type VI collagen, is a marker of endotrophin (a fragment of type IV collagen) and is linked to highly correlated to a “pro-fibrotic, pro-inflammatory and angiogenesis endotype” which clearly aligns with the biological mechanisms of galectin-3. This biomarker combination forms next-generation test for assessing the balance between scar formation and resolution, which may help guide therapeutic decision making and may help predict outcomes better than histology or imaging alone.
Big Pharma Eyeing Advanced Biomarkers for Fibrosis
Importantly, big pharma has taken notice of it. These biomarkers becoming more recognized for their diagnostic value and their regulatory and commercial potential. In fact, the $1.2 billion (upfront) acquisition of Boston Pharmaceuticals’ lead MASH asset by GSK (GSK) was reportedly driven in part by these compelling fibrosis biomarker data, which apparently correlated with treatment response and validated the clinical promise of the drug candidate. Nordic Bioscience, a leader in ECM biomarker development, has pioneered the commercial availability and standardization of these assays, working with partners across the biopharma landscape. Roche (RHHBY), for example, has integrated Nordic’s ECM biomarkers into its automated COBAS platform, which is an in vitro diagnostic platform that covers a broad range of testing solutions.
Madrigal and Akero, despite having the resources and access to patient samples, have not publicly reported any PRO-C3, PRO-C6, or CTX-III data, though Nordic currently has some efruxifermin data available on their website. This omission is somewhat conspicuous, especially as both companies target fibrotic NASH and have conducted trials that almost certainly collected serum samples capable of supporting these analyses. Their decision to withhold or delay such data may reflect concerns about variability, signal dilution in mixed-stage populations, or lack of robust antifibrotic effect in F4 patients. Either way, it places them at a disadvantage compared to developers like Galectin and Boston Pharma who are embracing biomarker-guided models of development.
In terms of which of these advanced biomarkers are most informative for F4 cirrhosis has yet to be fully elucidated. PRO-C3 captures ongoing fibrogenesis in patients who still have an active scar-generating phenotype. PRO-C6 is particularly valuable for understanding vascular remodeling, which contributes to portal hypertension and variceal development. And CTX-III, by indicating ECM turnover, is essential for distinguishing patients whose fibrosis is regressing from those merely plateauing. For trial design and clinical decision-making in F4, using all three together provides a real-time dynamic signature of fibrotic momentum, allowing for patient stratification, early efficacy signals, and a more refined understanding of drug mechanism.
There is some preclinical evidence that blocking galectin-3 may also have a positive effect on fibrolysis, by reducing TIMP expression, allowing MMPs (e.g., MMP-9) to degrade collagen more effectively, including collagen type III, thus increasing CTC-III neo-epitope levels, by decreasing collagen cross-linking, making ECM more susceptible to degradation, and by reducing fibronectin and laminin deposition, indicating less ECM stabilization and increased fibrolytic potential.
Dynamic ECM biomarkers like PRO-C3, PRO-C6, and CTX-III are ushering in a new paradigm for cirrhosis research and treatment, offering actionable insights that static histology and imaging cannot match. Belapectin’s pending biomarker data paired with clinical outcomes like variceal prevention will position it uniquely for regulatory engagement. As the FDA and EMA move away from relying solely on biopsy endpoints, and as pharma investors increasingly demand real-world, longitudinal disease metrics, these biomarkers are no longer optional they will be central to the future of MASH and fibrotic disease drug development.
Market Dynamics: The Short Squeeze Appears Underway
In the period before and after the release of topline NAVIGATE interim data, Martin Shkreli, offered uninformed and dismissive YouTube commentary on Galectin Therapeutics. Shkreli is an ex-pharmaceutical exec who is permanently barred from working the industry following his conviction for securities fraud ($64 million disgorgement), resurfaced in what some consider a predictable fashion to offer uninformed and dismissive YouTube commentary on Galectin, probably because this is the only way he can continue to engage in the healthcare industry—without being directly involved.
Although ex-con Shkreli lacks respect in the industry, has no current standing in the industry and is barred from working in it, he used his social media platforms to cast doubt on the drug’s efficacy. His commentary on YouTube was flippant and uninformed, exemplifying performative contrarianism instead of expertise. Nonetheless, his remarks found traction among a subset of retail speculators and short sellers that appear more interested in echoing his cynicism and piling on a bandwagon rather than interpreting data from the perspective of the FDA.
This manufactured skepticism, though loud, was devoid of substance and failed to grasp even the basic clinical significance of MASH cirrhosis or belapectin’s proven, statistically significant outcomes in a population with no current pharmacological treatment solutions, and eventual prognosis of early death. What emerged was not legitimate scientific discourse but rather a misguided smear effort that says more about the messenger than the medicine. The silver lining whas that this smear campaign gave long-term investors with high conviction the opportunity to buy additional shares at a steep discount after a pivotal data release.
Upside Opportunity
Galectin’s lead compound, belapectin, targets cirrhosis due to MASH. Unlike Akero’s EFX (an FGF21 analog targeting earlier-stage fibrosis) or Madrigal’s resmetirom (targeting fat resolution and primarily earlier fibrosis), Galectin’s NAVIGATE Phase 2b/3 trial focused exclusively on compensated F4 cirrhosis with portal hypertension, the most urgent and underserved patient population. They showed the first clinically meaningful effect in a cirrhosis trial. Given the absence of any approved drug for this population, analysts estimate belapectin could reach peak global sales of $18 billion over its exclusivity period, an estimate recently revised upward, presumably based on recent literature suggesting 5 million MASH patients will progress to cirrhosis, of which 3.3 million will have CSPH. Akero and Madrigal target the same MASH disease but in earlier fibrosis stages and without direct clinical benefit in cirrhosis or portal hypertension. Their valuations, however, are over 40-70x higher than Galectin’s, despite Galectin targeting the only population at imminent risk of decompensation. Furthermore, the FDA has no approved drug for cirrhosis, offering belapectin a potential path to conditional approval under accelerated frameworks.
Robust Insider Ownership: Management and Shareholders’ Goals Aligned
It should be noted that Galectin Therapeutics (GALT) is characterized by deep insider ownership and long-term alignment between management and shareholders, with over 50% of the company’s voting power controlled by insiders and affiliated parties. Chairman Richard Uihlein—the billionaire industrialist and co-founder of Uline—alone controls over 44 million shares, representing approximately 46.1% of the company, through a combination of direct equity holdings, convertible notes, and warrant instruments.
Galectin’s other major stakeholder is Jim Czirr, co-founder of Galectin and one of its earliest advocates, who beneficially (partially through the 10-X Fund) controls nearly 13 million shares.
Galectin’s CEO, Joel Lewis, has further reinforced this shareholder alignment by taking 80% of his compensation in equity over multiple years. Before joining Galectin, its important to note that Lewis served as financial manager of Richard Uihlein’s family office, which adds a layer of fiduciary trust between the company’s leadership and its largest shareholder.
Along with Uihlein’s and Czirr’s ownership, these three positions create an extremely tight float.
Financial Support of Galectin
It is often misunderstood or misrepresented in public discourse, including message boards, investment websites, and other media, that Galectin faces near-term financial strain due to its modest cash position reported on quarterly and annual financial statements. In reality, the company’s balance sheet has been uniquely fortified by the ongoing financial support of the company’s Chairman, Richard Uihlein, who has repeatedly demonstrated a willingness and desire to fund operations on terms quite favorable to the company and its common stockholders. This quite unusual degree of backing from a committed billionaire insider all but ensures that Galectin remains in a strong financial position. Consequently, the company is capable of advancing belapectin without the same capital constraints experienced by biotech peers with balance sheets that look like Galectin’s.
The Ongoing Rally or Short Squeeze Could Continue
Galectin Therapeutics currently had approximately 8.67 million shares sold short as of the writing of this article (a few weeks ago), accounting for 19.84% of its public float. The days-to-cover ratio exceeds 40, and the annualized cost to borrow has surged above 54% recently, an unusually high figure that underscores the intensity of bearish positioning. With daily trading volume remaining thin and more than 50% of shares controlled by insiders and long-term retail holders, the stock’s float is exceptionally illiquid.
The past week has shown this to be a precarious setup for short sellers. These short sellers appear to have now covered their positions. Alternatively, they may be currently trapped in their short position. A significant catalyst like a licensing deal, fibrosis biomarker data release, or positive communication from the FDA could drive the continuation of this apparent aggressive short squeeze and usher in new longs. The conviction among Galectin’s shareholder base, paired with the drug’s promising efficacy in a high-unmet-need population, further compounds this pressure. In short, the setup suggests that a significant revaluation event may not only be possible—but also imminent.
Conclusion
Galectin Therapeutics is undervalued and misunderstood by Wall Street, partially due to short-and-distort tactics, but also because of a general lack of nuanced understanding of MASH cirrhosis and its clinical management by the investment community. With shares tightly held by insiders, a potential conditional approval, $18B in estimated annual peak sales (about 200x the company’s current market capitalization) in the U.S. alone for just MASH cirrhosis with CSPH, advanced biomarkers data set to be released, and short interest high with no public stock offering in sight for shorts to cover, the shares appear both extremely undervalued and ripe for a continued short squeeze.
More By This Author:
Intelligent Bio Solutions’ Fingerprint Drug Screening Technology Poised For Massive Growth
MAIA Biotechnology: Undervalued With Eye-Popping Cancer Data And Partnership Potential


Comments
Log in or sign up to join the conversation.