
RedHill's R&D Day Highlights Potential For Bekinda
On April 27, 2017, RedHill Biopharma Ltd (NASDAQ: RDHL) held an R&D Day highlighting for investors the clinical and commercial attributes of BEKINDA® (RHB-102). BEKINDA is an oral, extended-release, once-daily formulation of the antiemetic drug ondansetron. The drug is currently being examined as a treatment for acute gastroenteritis and gastritis in a Phase 3 clinical trial known as the GUARD study. GUARD completed enrollment in February 2017 and top-line data are expected in June 2017. A separate Phase 2 study investigating the drug as a treatment for diarrhea-predominant irritable bowel syndrome (IBS-D) is also ongoing, with top-line data expected in the third quarter 2017.
Quick Background on BEKINDA®
BEKINDA is an oral, bi-modal, extended-release, once-daily formulation of the antiemetic drug ondansetron. Ondansetron is a selective serotonin 5-HT3 receptor type antagonist originally approved in January 1991 and sold under the brand name Zofran® by GlaxoWellcome Inc. for the prevention of chemotherapy and radiation-induced nausea and vomiting, and the prevention of postoperative nausea and vomiting. Zofran® sees significant use in the prevention of nausea and vomiting, largely due to the drug's benign safety profile and general utility in preventing emesis. The patent expired in December 2006, but not before the drug achieved peak sales that year of $1.7 billion.
The recommended dose of ondansetron for the prevention of radiation-induced nausea and vomiting is one 8 mg tablet one to two hours before therapy, then 8 mg orally every eight hours for five days post-treatment. For prevention of chemotherapy-induced nausea and vomiting, patients are recommended to take 8 mg twice daily. Peak plasma concentration occurs approximately 90 minutes following oral administration. The half-life is approximately 3-4 hours.
RedHill's BEKINDA is a once-daily oral formulation of ondansetron designed to provide ease of use and greater patient compliance over the generic twice-daily formulation. The graph below shows the pharmacokinetic comparison between Zofran® (ondansetron) and BEKINDA. BEKINDA offers virtually identical onset of action to the standard 8 mg Zofran® tablet, but with superior TMAX and AUC that allows for once-daily dosing. The data also shows a low coefficient of variance among patients.
(Click on image to enlarge)
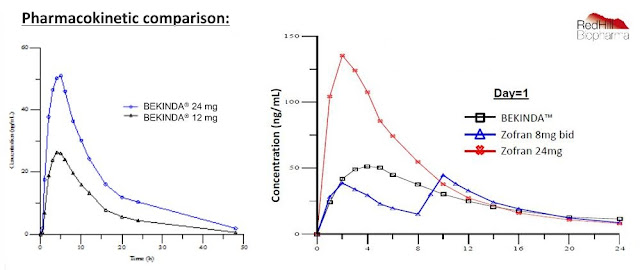
RedHill has developed a 24 mg dose of BEKINDA for acute gastroenteritis (GE) and a 12 mg dose of BEKINDA for IBS-D. The company recently received a notice of allowance for two additional patents on BEKINDA in the U.S. that will protect the IP until at least 2034.
BEKINDA for Acute Gastroenteritis / Gastritis
Gastroenteritis (inflammation of the stomach and small intestine) and gastritis (inflammation of the stomach) are often simply referred to as "stomach flu". The primary symptoms are vomiting and diarrhea, both of which can lead to additional symptoms, including abdominal pain and dehydration. Although colloquially referred to as "stomach flu", gastroenteritis is not caused by the influenza virus, as influenza only attacks the respiratory system. Instead, the two most common culprits of gastroenteritis are the rotavirus and norovirus. Other viruses that may cause gastroenteritis are the astrovirus, sapovirus, and enteric adenovirus. Gastroenteritis can also be caused by bacterial or parasitic infection, in which case symptoms will also likely include low-grade fever and muscle ache, with the most common pathogens being enterotoxigenic E. Coli, Clostridium difficile, salmonella, and giardia.
Despite the fact that the label only notes prevention of chemotherapy and radiation-induced nausea and vomiting and prevention of postoperative nausea and vomiting, ondansetron sees significant use in the emergency room (ER) for acute gastroenteritis (GE). In fact, ondansetron ranks as one of the most commonly prescribed drugs in the ER in the U.S., with over 20 million doses prescribed in 2013 according to the CDC's National Center for Health Statistics. Unfortunately, the short half-life of the generic formulation limits effectiveness and compliance. RedHill's BEKINDA is designed to provide a more convenient and longer effective option, which is particularly attractive for the outpatient market.
A total of 330 patients enrolled in GUARD, randomized 60:40 to BEKINDA vs. placebo. The final patient is now off the drug and the data are being analyzed. RedHill noted during its R&D Day that no adverse safety signals have been noted during the trial. Top-line data are expected in June 2017. I conducted a statistical analysis of the efficacy of ondansetron using historic data in this indication and believe the trial has an excellent chance at success >> see my analysis here.
- Opportunity in GE -
Gastroenteritis affects an enormous number of Americans each year. According to the U.S. CDC estimated 19-21 million people in the U.S. get infected with norovirus and develop acute gastroenteritis each year. This leads to 1.7-1.9 million outpatient visits and 400,000 ER visits per year. Severe cases result in 56,000-71,000 hospitalizations and 570-800 deaths, mostly among young children and the elderly each year. And although the norovirus is the number one cause of acute gastroenteritis in the U.S., it still only accounts for 21% of the cases. Doing the math, one can back-calculate that there are likely over 100 million episodes of acute gastroenteritis in the U.S. each year. In fact, RedHill presented numbers at its R&D Day noting 179 million cases in the U.S. each year (see below).
(Click on image to enlarge)

The company estimates that 10% of these cases seek medical attention, the majority of which are treated by hydration, probiotics, antibiotics, antispasmodics, and antiemetics, resulting in about 1.5 million prescriptions per year and $3.1 billion in direct medical expenses associated with these medications. The efficacy of generic ondansetron is well documented in this setting. The majority (~75%) of the generic ondansetron tablets are given in the emergency department, with 25% given the medication at discharge. RedHill believes antiemetics, a category dominated by ondansetron, generate $1.0 billion in sales (at generic pricing) in acute gastroenteritis.
It seems logical that RedHill's BEKINDA, a rapid-acting and long-lasting formulation designed to improve compliance and eliminate the need for return visits to the ER, could gain meaningful share. In fact, it might make sense for the company to create a BEKINDA "dose pack" that can be given to the patient to take home to prevent the need for a returned visit to the ER. With modest pricing and good formulary coverage, BEKINDA looks like a $250-300 million opportunity in the U.S.
BEKINDA for IBS-D
IBS is an idiopathic GI disorder characterized by abdominal pain and altered bowel habits. IBS can have unpredictable and significant impacts on quality of life. It is highly prevalent and estimated to affect between 5% and 30% of the U.S. population, or around 35 million people - mostly women - according to published data. There are three subtypes of IBS, diarrhea-predominant (IBS-D), constipation-predominant (IBS-C), and mixed (IBS-M). The CDC estimates that 40-60% of all IBS cases are IBS-D. Depending on the diagnosis, different medications are prescribed to treat the symptoms of the disease.

There is a clear scientific rationale for the use of a selective serotonin 5-HT3 receptor type antagonist in this indication. In fact, Lotronex® (alosetron) is approved for IBS-D, but with restrictions due to severe toxicities. Pilot studies of existing formulations of ondansetron have demonstrated utility in treating IBS-D. 5-HT3 receptor antagonists, like alosetron and ondansetron, are used to suppress the excessive activity of serotonin receptors in the gut. Importantly, ondansetron does not show the same types of tolerability issues evident with alosetron.
A Phase 2 clinical study with BEKINDA (12 mg) is currently ongoing examining the drug as a treatment for IBS-D. Target enrollment was 127 patients at 16 clinical centers in the U.S. The primary endpoint is a response in stool consistency as compared to baseline, per FDA guidance definition. Patient enrollment completed in April 2017 and top-line data are expected in the third quarter 2017.
- Opportunity in IBS-D -
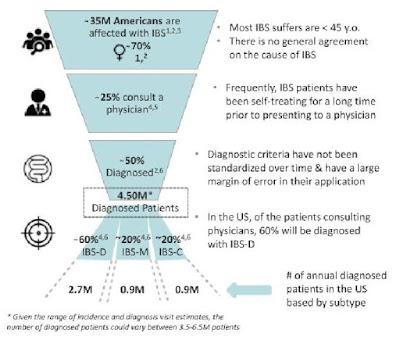
About 9 million individuals in the U.S. seek medical treatment for IBS, resulting in over $20 billion in direct and indirect medical costs each year. A RedHill's R&D Day, the company presented the slide below noting roughly 4.5 million individuals in the U.S. with a diagnosis of IBS, approximately 2.7 million of which have IBS-D. Data from Symphony / Foster Rosenblatt pegs the IBS market at 4.2 million prescriptions per year, generating $1.8 billion in sales in 2016. The majority of the market today is in IBS-C, dominated by the launch of Allergan's oligo-peptide guanylate cyclase-C (GC-C) agonist, Linzess® (linaclotide), in 2012.
(Click on image to enlarge)
However, the IBS-D market is expected to grow rapidly in the coming years now that there are two new drugs recently approved for this specific subtype of IBS. These drugs are Allergan's Viberzi® (eluxadoline), a μ-opiod receptor agonist / d-opioid receptor antagonist used to down-regulate the concentration of serotonin in the gut and Valeant's Xifaxan® (rifaxmin), a non-absorbed, broad-spectrum antibiotic that alters the gut flora.

Given that BEKINDA® presents a different, yet proven, mechanism of action from Viberzi and Xifaxan, it will be interesting to see what kind of market share RedHill can capture once approved. Both Viberzi and Xifaxan have non-preferred formulary status. Viberzi costs $8,000+ per year; Xifaxan, which is limited to three treatments per year, costs over $4,000 per year. During the company's R&D Day presentation, RedHill made the point (a few times) that the cost of good on BEKINDA are very low and that pricing may be an advantage versus the more expensive competition. With 10% market share and pricing at $2,500 per year (my guess), BEKINDA is a potential $675 million drug.
Conclusion
Management has previously announced that they believe the Phase 3 GUARD study may be sufficient to support a potential marketing application in the U.S. Of course, this is dependent upon strong data and further guidance from the FDA. That makes the pending Phase 3 data an important catalyst to watch for RedHill investors in the next few weeks. I see BEKINDA as a $250-300 million drug in acute gastroenteritis for RedHill.
The opportunity in IBS-D is larger and more attractive in my opinion. Just 10% market share generates $675 million in potential sales for BEKINDA. Allergan is obviously a major player in IBS-D with Linzess and Viberzi. BEKINDA, with a different and proven mechanism of action, might be a nice addition to Allergan's portfolio. Likewise, Valeant, a company that RedHill already has a partnership with for Phase 3 ready bowel prep drug, RHB-103, is the other big player in IBS-D with Xifaxan. Prescriptions of Xifaxan are limited due to the potential for antibiotic resistance to develop to the generic formulation, which is an important antibiotic used to combat traveler's diarrhea and C. difficile infection. BEKINDA might make an attractive additional to Valeant's IBS portfolio and allow the company to compete more effectively against Allergan.
Other late-stage assets at RedHill, including Phase 3 RHB-104 for Crohn's disease and RHB-105 for H. pylori infection, round out an impressive GI-focused pipeline. RedHill also now promotes two commercial products, Donnatal® for IBS and EnteraGam® for chronic diarrhea that further strength the core focus on GI and make RedHill an attractive emerging specialty pharma story for long-term investors.
Disclosure: Please see important information about BioNap, Inc. and our relationship with names in this article in our more


