
Why I'm Long Shares Of HedgePath Pharma
TM editors' note: This article discusses a penny stock and/or microcap. Such stocks are easily manipulated; do your own careful due diligence.
I am long shares of HedgePath Pharmaceuticals (HPPI) because I believe the stock represents a compelling investment opportunity at today's price. HedgePath is a biopharmaceutical company developing an improved formulation of itraconazole for the treatment of Basal cell carcinoma nevus syndrome (BCCNS). The drug, called SUBA™-Cap, is currently being investigated in a Phase 2b clinical trial. Preliminary data from the study reported in October 2016 look excellent and the potential exists that HedgePath may be in a position to seek U.S. FDA approval upon successful completion of the Phase 2b study pending final results expected later in 2017.
Below is a comprehensive review of HedgePath Pharma for investors.
Basal Cell Carcinoma Nevus Syndrome (BCCNS)
Basal cell carcinoma nevus syndrome (BCCNS) also referred to as nevoid basal cell carcinoma syndrome or Gorlin-Goltz syndrome, is an autosomal dominant disorder characterized by the early appearance of basal cell carcinomas (1). Non-hereditary, sporadic basal cell carcinoma (BCC) is the most common type of human cancer in the U.S., and it usually occurs as a result of prolonged exposure to sunlight. It is most frequently found in people over age 45 and curable if found early.
Conversely, individuals with BCCNS develop multiple basal cell carcinomas at an early age and continue to develop new tumors throughout their lifetime. Other distinguishing clinical features found in the majority of patients with BCCNS include keratocystic odontogenic tumors of the jaw, craniofacial defects, ectopic calcifications, bifid ribs, and dyskeratotic palmar and plantar pitting (2). These are specific to nevus syndrome patients resulting from the generic disorder and not found in otherwise healthy individuals with sporadic BCC.
Nevertheless, what investors need to understand is that BCCNS manifests as dozens or hundreds of BCC tumors, at an early age, and is the direct result of a hereditary mutation in the tumor suppressor gene PTCH1 and not exposure to sunlight or harmful UV radiation. Importantly, early diagnosis of BCCNS is critical for possible prevention of the devastating effects of BCC tumors and the establishment of multidisciplinary care (3).

Basal cell carcinoma, whether sporadic or hereditary, is caused by defects in hedgehog signaling which result in constitutive pathway activity and tumor cell proliferation (4, 5). As noted above, molecular analysis studies suggest a relationship between BCC and the loss-of-function mutations of the patched gene (PTCH) found on chromosome arm 9q (6). PTCH1 is a member of the patched gene family and is the receptor for sonic hedgehog (SHh), a secreted molecule implicated in the formation of embryonic structures and in tumorigenesis (7). The gene functions as a tumor suppressor, and the PTCH1 gene product is a transmembrane protein that suppresses the release of another protein called Smoothened (SMO). When SHh binds PTCH1, SMO is released and signals cell proliferation by activation of the Gli family of transcription factors.

Clinical experiments with hedgehog inhibitors have shown real promise in halting and even reversing the growth of various tumor types, including basal cell carcinoma (8, 9), prostate cancer (10, 11), non-small cell lung cancer (12, 13), pancreatic cancer (14), and other solid tumors (15, 16). From a commercial standpoint, the U.S. FDA approved the first hedgehog pathway-targeted small molecule, Roche's Erivedge® (vismodegib) in January 2012 (17). Erivedge is approved for the treatment of adults with metastatic basal cell carcinoma (mBCC), or with locally advanced basal cell carcinoma (laBCC) that has recurred following surgery or who are not candidates for surgery or radiation (18).
Treatment for BCCNS - Surgery, After Surgery, After Surgery...
There are several treatment options available to patients with BCCNS. These options include:
Excision: Excision is the surgical removal of the cancer lesion performed by a dermatologist, otolaryngologist (ear-nose-throat specialist), plastic surgeon, or another specialist. If the lesion is large enough, a skin graft from another area of the body may be required, with a goal to minimize scarring and disfigurement. While this certainly is the simplest way to deal with the skin cancer lesions, it has a higher rate of recurrence than some other treatments and becomes more difficult with the removal of larger lesions.
Excision also presents specific challenges when the tumors are located on the face or neck. Many BCCNS patients report reduced quality of life and long-term emotional and physical stress due to facial BCCNS tumors or scarring from surgical excision (19).
Mohs Surgery: Mohs micrographic surgery is a more advanced form of excision in that the excised area tends to be larger than just the cancerous area and includes a margin of healthy cells surrounding the lesion. Mohs surgery is more effective than traditional surgical excision (20); however, it’s also usually more costly, complex, and time-consuming and can cause disfigurement (21, 22). This is the standard of care for BCC lesions.
Electrodesiccation and Curettage: ED&C utilizes a light electric current to dry out and kill cancerous cells, which are scraped away using a round knife called a curette. This process is repeated several times until the entire lesion has been removed, along with a margin of healthy skin to ensure complete removal (23). It is performed under local anesthetic. ED&C involves little bleeding and requires no stitches, but it takes longer to heal and may not be suited for patients with dozens or hundreds of BCCNS tumors.
Cryosurgery: Almost the opposite of ED&C, cryosurgery freezes the skin cancer lesion with liquid nitrogen instead of burning it. The growth scabs over and usually falls off within a couple of weeks. Cryotherapy has a lower cure rate than other procedures, but it is the procedure of choice for people with bleeding disorders or trouble with anesthesia.
Topical Chemotherapy: Topical chemotherapy involves applying the drug directly to the cancerous lesions as a cream. The cancerous cells absorb the drug and die off, forming scabs that can be removed. Side effects include temporary skin irritation, but the area tends to heal with the least amount of scarring. However, the treatment may miss portions of some tumors that lie deeper under the skin and for patients with dozens of BCCNS tumors topical chemotherapy becomes inefficient.
Photodynamic Therapy: PDT uses a drug that only becomes active under a certain wavelength of light. Cancerous cells absorb the drug more readily than healthy cells, so the cancerous cells are killed off while the healthy cells remain. The procedure can be made more accurate by using lasers to direct the light only at the cancerous cells. Patients sometimes complain of feeling “cigarette burns” or other irritation, and they must stay out of the sun for the next day or two, but PDT can be very useful for treating many BCCs at one time.
The Patient Perspective
I recently spoke with Kristi Schmitt Burr, Executive Director of the BCCNS Life Support Network. The non-profit organization is dedicated to providing counseling and support services to children and adults with BCCNS. From what I've seen, they do fantastic work and Ms. Burr provided me with a wealth of information on what life is like as a sufferer of BCCNS. I encourage readers to donate and help support their work >> link (I sent them a donation on March 21st).
After speaking with Ms. Burr, I learned a great deal about the challenges of being a BCCNS patient. Surgery upon surgery is the norm. Severely affected patients might undergo multiple procedures on a weekly or monthly basis; and, because of recent changes to healthcare laws, often the reimbursement for the number of tumors that can be excised at one time is limited. This is because there are no CPT codes for removal of BCC tumors specific to BCCNS patients. Current procedural codes cover the removal of up to three BCC tumors at a time; perfectly adequate and reasonable for a patient with sporadic BCC that might seek the removal of one or two tumors in their lifetime. However, a BCCNS patient might seek removal for dozens of tumors a month, making it nearly impossible for the current reimbursement protocol to keep up with the demands of the disease. It's a square peg in a round hole.
Additionally, Mohs surgery and things like PDT only treat the symptoms of each individual tumor. They do not prevent recurrence or the formation of new tumors. Recall, BCCNS patients are making hundreds of tumors a year and surgery does not treat the underlying disease for the BCCNS patient. For individuals with sporadic BCC, this is fine because there is no underlying disease. This is not the case for BCCNS. Ms. Burr told me the ideal treatment option would be a systemic product that targets the underlying condition and reduces the morbidity and mortality associated with the disease. BCCNS patients are desperate for a solution that reduces the cost and emotional hardships that stem from continued surgery after surgery that often leads to disfigurement. An effective medication that shrinks existing tumors and reduces the incidence of new tumor formation, with limited side-effects, would vastly improve the quality of life for BCCNS patients.
Erivedge® for BCC - An Imperfect Option
Erivedge (vismodegib) is an oral small molecule inhibitor of the Hedgehog pathway (Hh) signaling. Erivedge use in mBCC and laBCC is growing compared to invasive procedures noted above - market share was found to be as high as 40% in a recent study published in JAMA Dermatology (24). Roche posted global sales of Erivedge of CHF203 million ($204 million) in 2016, up 21% from 2015 levels. Approximately 66% of these sales were derived from the U.S. market.
Approval of Erivedge was based on a Phase 2, international, single-arm, multicenter, open-label, 2-cohort trial conducted in 104 patients with either metastatic basal cell carcinoma (mBCC) (n = 33) or recurrent locally advanced BCC (laBCC) (n = 71). The median age of the efficacy evaluable population was 62 years. Patients received 150 mg vismodegib per day orally until disease progression or unacceptable toxicity. The primary efficacy outcome was objective response rate (ORR) as assessed by an independent review facility (IRF).
Of the 104 patients enrolled, 96 patients (92%) were evaluable for ORR. For the mBCC cohort (n = 33), 97% of patients had prior therapy including surgery (97%), radiotherapy (58%), and systemic therapies (30%). For the laBCC cohort (n = 63), 94% of patients had prior therapies including surgery (89%), radiotherapy (27%), and systemic/topical therapies (11%). The median duration of treatment was 10.2 months (range 0.7 to 18.7 months). Efficacy results published in the New England Journal of Medicine show an ORR of 30.3% for mBCC and 42.9% for laBCC (25). Complete response (CR) rates for mBCC and laBCC were 0% and 20.6%, respectively. Partial response (PR) rates were 30.3% and 22.2%, respectively. Median response duration was 7.6 months for both mBCC and laBCC.
Adverse events in the trial were significant and included muscle spasms (65%), alopecia (61%), dysgeusia (49%), weight loss (44%), fatigue (34%), nausea (28%), loss of appetite (22%), and diarrhea (21%). Several grade 3/4 events, including muscle spasms, weight loss, and fatigue were reported.
- Erivedge® for BCCNS -
Roche conducted a separate Phase 2 trial with Erivedge in patients with BCCNS. The trial enrolled 41 patients with BCCNS, randomizing 2:1 to 150 mg vismodegib or placebo for a planned 18 months. During the study period, investigators tracked more than 2,000 existing and 694 new surgically eligible basal-cell carcinomas. The primary statistical endpoint was the comparative rate of appearance of new basal cell carcinomas (SEB) that were eligible for surgical resection.
A total of 38 of the 41 patients (93%) completed at least three months of follow-up visits and had data for the primary endpoint. Published data in the NEJM show vismodegib significantly reduced the per-patient rate of new surgically eligible basal-cell carcinomas below that of the placebo group (P<0.001). Vismodegib also reduced the size of existing surgically eligible basal-cell carcinomas, expressed as the percent change from baseline in the sum of the longest diameters (mean, −65%, vs. −11% with placebo; median, −71%, vs. −21% with placebo; P=0.003) (26).
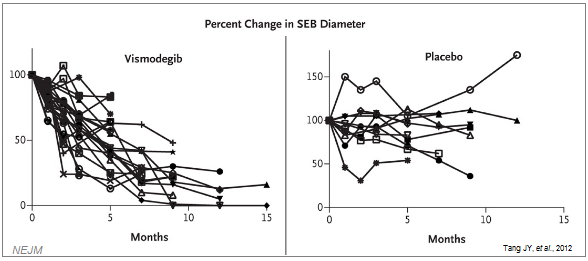
The vismodegib efficacy data are quite impressive. Unfortunately, BCCNS is a chronic disease and to achieve long-lasting disease control it is likely patients are going to have to remain on the drug for the rest of their lives. Follow-up analysis from the above trial found that 54% of the vismodegib patients had discontinued therapy at 12 months due to side effects. In fact, the mean duration was only eight months, and no patient was on the drug longer than 15 months. So while the efficacy data look excellent, Erivedge is simply not a viable long-term option for BCCNS patients.
Despite conducting the trial, Roche never has sought approval for Erivedge in BCCNS, likely due to the small patient population and lack of compelling long-term data. When I spoke to Ms. Burr at the BCCNS Life Support Network, she noted that some BCCNS patients do take Erivedge and that although the side effects are difficult, the drug is an imperfect solution to patients that have exhausted other options.
A Significant Unmet Medical Need
The lack of a truly effective pharmaceutical product leaves frequent excisions as the only viable long-term treatment option for BCCNS patients. As noted above, many BCCNS patients have dozens or even hundreds of tumors covering their back, shoulders, neck, and head. Excision surgeries are painful and inefficient. Scarring and disfigurement are significant sources of anxiety and emotional stress, and reimbursement is a major challenge for those suffering for BCCNS.
Itraconazole As A Cancer Therapy
Itraconazole (ITZ) is a triazole antifungal agent with widespread clinical use in the prevention and systemic treatment of a broad range of fungal infections, including aspergillosis, blastomycosis, candidiasis, histoplasmosis, and in some dermatological and nail infections. Common trade names include Sporanox® (Janssen) and Onmel® (Merz), although the drug is now widely available as a generic.
Recent evidence points to the potential utility of itraconazole as an anti-cancer agent. Work out of Stanford University and Johns Hopkins University shows the drug is a potent antagonist of the Hedgehog (Hh) signaling pathway that acts by a mechanism distinct from its inhibitory effect on fungal sterol biosynthesis (27). Kim J, et al. show that systemically administered Itraconazole, like other Hh pathway antagonists, can suppress Hh pathway activity and the growth of medulloblastoma in a mouse allograft model and does so at serum levels comparable to those in patients undergoing antifungal therapy. Mechanistically, itraconazole appears to act on the essential Hh pathway component SMO by a mechanism distinct from that of cyclopamine and other known SMO antagonists, and similar to that of Roche's Erivedge.
For example, a Phase 2a clinical study with itraconazole in patients with BCC published in the Journal of Clinical Oncology (28) and presented at AACR in April 2011 shows itraconazole reduced cell proliferation by 45% (P = 0.04), Hh pathway activity by 65% (P = 0.03), and reduced tumor area by 24% (95% CI, 18.2-30.0%). Tumors from untreated control patients and from those previously treated with vismodegib showed no significant changes in proliferation or tumor size. A total of 57 BCC tumors from eight patients were treated with itraconazole. Percentage change in tumor area for all 57 tumors is presented below. The results are quite impressive:

- Issues With Generic Itraconazole -
Dozens of other anti-cancer studies with itraconazole have been conducted with the generic formulation of the drug. The challenges for generic itraconazole as an anti-cancer agent include the poor bioavailability and inconsistent plasma levels, as well contraindications with achlorhydric agents and proton-pump inhibitors. Itraconazole is poorly soluble in water and has a mean absolute bioavailability of only 55% (29). Absorption of the generic formulation is also reduced by a mean of 20% by concomitant use of H2-antagonists cimetidine and ranitidine (30). It is contraindicated for use with a host of other drugs listed in the Prescribing Information (31). Additionally, fed / fast conditions have a major impact on the bioavailability, with fasting conditions increasing the bioavailability by up to 60% (32).
Enter HedgePath Pharmaceuticals
Mayne Pharma has licensed the U.S. commercial rights to SUBA-Itraconazole for the treatment of cancer to Tampa-based HedgePath Pharmaceuticals. Australian-based Mayne Pharma is a rapidly growing generic pharmaceutical company with a new focus on dermatology. They are the sole source supplier of SUBA-Itraconazole and seems an excellent collaborative partner for the company. In fact, Mayne owns significant equity in HedgePath - approximately 58% as of a recent SEC filing (33). Mayne also participated in a $5.5 million private placement by HedgePath in June 2016.
Mayne has developed a proprietary, patented drug delivery technology called SUBA™ designed to enhance the bioavailability of poorly soluble drugs. The technology achieves “super bioavailability” compared to conventional formulations (>90%) by utilizing a solid dispersion of API in a polymer to improve the absorption of drugs in the gastrointestinal tract. This dispersion improves the dissolution of poorly soluble drugs compared to their normal crystalline form, increasing bioavailability, reducing intra/inter-patient variability, and reducing side-effects (34).
Mayne has applied the SUBA technology to improve the bioavailability of itraconazole. Data from Mayne show SUBA-Itraconazole has 80-90% bioavailability compared to the 55% noted above for generic itraconazole and less variation in AUC at steady state (35). And since absorption is not dependent on stomach pH, SUBA-Itraconazole bioavailability is not materially impacted by fed / fast conditions and should not be contraindicated for use in achlorhydric patients (low acid stomach) or patients with acid reflux (requiring proton-pump inhibitors).
(Click on image to enlarge)

- SUBA™-Itraconazole -
HedgePath is currently enrolling patients in a Phase 2b open-label trial (NCT02354261) of SUBA-Itraconazole (SUBA-Cap) in subjects with basal cell carcinoma nevus syndrome (BCCNS). Target enrollment for the Phase 2b trial is 40 patients with active BCCNS. For each subject, 10 to 15 of the largest lesions are selected by the investigator at baseline to represent a valid sample of overall lesions (target tumors). The longest diameters of these target tumors are then added together to create a "target tumor burden” number.
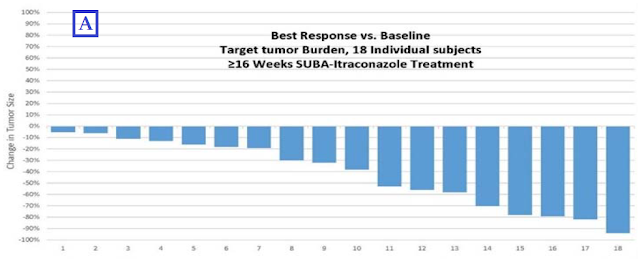
Because this is an open-label study, management has been able to provide ongoing updates from the trial to the market. The most recent update came in October 2016 and demonstrated impressive results for SUBA-Cap. Management conducted two separate interim analyses: (A) the change in target tumor burden for each subject (which is based on the change in the sum of the longest diameters of each subject’s target lesions) to measure the change in target tumor burden from baseline; and (B) the change in the longest diameter of all individual target lesions from baseline across all subjects in the study, which the company believes documents clinical impact.
On target tumor burden (A), among the 18 subjects who have dosed for ≥ 16 weeks, 100% of the patients had a target tumor burden reduction. Importantly, target tumor burden did not increase in any subject and was reduced by greater than 30% in 11 of the 18 subjects (61%) with an average reduction of 61%. The results of the best response vs. baseline for each patient are graphed below:
(Click on image to enlarge)
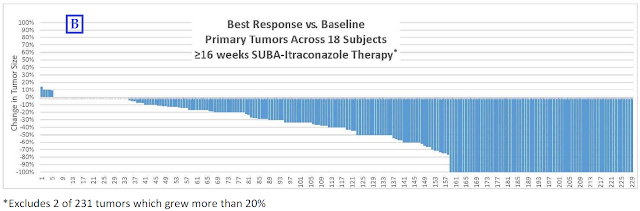
On changes in the longest diameter of individual target lesions (B), the company conducted an interim analysis of 231 individual target lesions across all 18 subjects. All of these tumors were primary tumors, meaning none were metastatic lesions. The interim analyses showed that 31% of cancerous lesions have disappeared (complete response), an additional 30% have exhibited greater than a 30% reduction but less than 100% (partial response), and 38% have remained stable (< 20% increase and < 30% reduction). Presented below are the results of the 229 tumors that demonstrated stable disease, partial response and complete response:
(Click on image to enlarge)
These results compare very well to the aforementioned Erivedge. However, given the similar mechanism of action, it is already expected that SUBA-Cap would offer up impressive efficacy data similar to that of Erivedge. As noted above, the efficacy of Erivedge is not the issue; the issue is the side effect profile and that fact that patients with BCCNS suffer from life-long chronic disease and simply cannot tolerate being on Erivedge for longer than eight months.
This does not seem to be an issue with itraconazole, even with the non-optimized generic formulation of the drug. I found several studies that report excellent long-term tolerability of itraconazole when used prophylactically as an antifungal agent. For example, an independent study out of Hamanomachi Hospital in Japan showed that 200 mg/day of itraconazole is well tolerated as a prophylactic in immunocompromised patients with hematological malignancies (36). A separate study conducted at Royal Prince Alfred Hospital in Australia found that 400 mg/day itraconazole is effective and well-tolerated as a prophylactic in patients with relapsed acute myeloid leukemia (37). Itraconazole is also commonly used as a maintenance prophylactic to prevent histoplasmosis in patients with AIDS (38). If the drug is safe enough for long-term use in AML and AIDS patients, it is likely safe enough for long-term use in patients with BCCNS.
What's Next For HedgePath?
Data for SUBA-Cap demonstrate impressive interim Phase 2b results for HedgePath Pharma. Target enrollment is 40 patients and as per the company's Form 10K in February 2017, 13 subjects have completed 24 or more weeks. Per the protocol, 33 subjects must complete 16 weeks of active dosing, with 30% showing a response rate. This equates to only 11 patients. In October 2016, management reported that 11 patients have responded with only 18 subjects completing 16 weeks. Obviously, the trial needs to continue, but I find it extremely encouraging that HedgePath has already achieved the target number of responders for the study to be successful. Perhaps the most important takeaway from the interim Phase 2b results is that SUBA-Cap compares very favorably with Erivedge on efficacy and safety.
HedgePath management intends to continue collecting data and will interact with the U.S. FDA regarding ongoing results demonstrating efficacy and tolerability for SUBA-Cap treatment for BCCNS. Erivedge and Odomzo are not approved for BCCNS, which presents HedgePath the opportunity to petition the FDA for approval if the final results of this 40-patient trial are as encouraging as the interim data above. As noted above, the company may have already achieved the primary endpoint with still half the patients left to fully treat for 16 weeks. Nevertheless, there can be no assurance that this trial will enable an NDA filing.
How Big Is SUBA-Cap?
The U.S. National Institute of Health estimates approximately one million individuals in the U.S. will develop BCC in 2016; however, less than 1% of these will be Nevus / Gorlin syndrome patients (39). This equates to roughly 10,000 patients in the U.S. Work done by Evans DG, et al. in 1991 estimated the incidence rate in the UK at 1 per 57,000 (40), which would equate to roughly 6,000 in the U.S. assuming similar etiology among the two countries. Evans DG, et al. updated this figure in 2010, revising the estimate to 1 per 30,827 (41), again which would equate to roughly 10,300 patients in the U.S. assuming similar etiology.
Management has been using the 10,000 figure in its SEC filings and most recent investor presentation (42). That being said, the market is likely significantly larger than just BCCNS patients. For example, there are an estimated 4 million cases of BCC diagnosed in the U.S. A significant number of BCC patients undergoing surgical treatment for facial tumors (excisions) in the U.S. will require reconstructive surgery following excision of their tumors. Some of these surgeries might benefit from pretreatment with SUBA-Itraconazole to reduce the size of the tumor (see the Phase 2a data noted above) or benefit from post-surgical treatment with SUBA-Itraconazole to reduce the incidence of recurrence. The company has not determined if it will seek an approved indication for sporadic basal cell carcinomas.
In June 2016, the U.S. FDA granted HedgePath's SUBA-Itraconazole Orphan Drug designation for the treatment of BCCNS (43). I believe this is a significant market opportunity for HedgePath. Roche's Erivedge costs roughly $10,800 per month (44), with the average patients on the drug for 7-8 months. In 2015, Novartis gained approval for Odomzo® (sonidegib). Odomzo is a hedgehog pathway inhibitor indicated for the treatment of adult patients with laBCC that has recurred following surgery or radiation therapy, or those who are not candidates for surgery or radiation therapy. Novartis sold the rights to Odomzo to Sun Pharma in late 2016 for $175 million upfront plus future milestones and royalties. The drug costs $10,400 per month (45). Importantly, neither of these drugs is approved for the treatment of BCCNS.
I believe that SUBA-Itraconazole is a share gainer in BCC and BCCNS given the drugs solid efficacy and substantially reduced toxicity / better tolerability than Erivedge and Odomzo. Market research suggests an effective price between $4,000 and $5,000 per month for SUBA-Itraconazole. I believe the drug has pricing power higher than this, but even at only $5,000 per month, the market opportunity for HedgePath is $375 million in BCCNS. In BCC, assuming 25% of the patients might opt for adjunct pharmacotherapy pre- or post-surgery, the market is another $600 million.
Final Thoughts
HedgePath remains an attractive story for small-cap biotech investors. The company is likely to report positive top-line Phase 2b results during the first half of 2017. As noted above, the company has already seen the required number of responders in the Phase 2b study to hit the FDA benchmark for success. If the full data look as strong as the interim data presented in October, I expect the company to begin the filing process in 2017 to seek U.S. FDA approval for SUBA-Cap via the 505(b)(2) pathway in 2018.
I see the peak opportunity for SUBA-Cap at $750 million, which includes the upside from use in metastatic or locally advanced BCC, or other solid tumors where itraconazole has demonstrated utility such as lung cancer or prostate cancer. The current market value of the company is only $85 million and Mayne Pharma owns over 58% of the shares. I also like the fact that insiders own another 32% of the company!
For a company with a potential $750 million drug 18 months from approval, $85 million is an incredible bargain. I can easily see HedgePath being worth $200 million based on the fundamentals today (about what Sun Pharma paid for Odomzo in December 2016) and over $500 million in 2018 if SUBA-Cap gains approval. A good comparison for investors is Curis, Inc. (NASDAQ: CRIS), Curis was the original inventor of vismodegib before it licensed the product to Genentech in 2003. Curis has a PI3K/HDAC inhibitor for DLBCL currently in a Phase 2 clinical trial and a PDL1/VISTA antagonist in a Phase 1 clinical trial for advanced solid tumors. The company's market value is $425 million, 5X that of HedgePath today!
Disclosure: Please see important information about BioNap and our relationship with companies mentioned in this article in our more


