
BriaCell Phase 1/2a Trial Underway
TM editors' note: This article discusses a penny stock and/or microcap. Such stocks are easily manipulated; do your own careful due diligence.
On March 15, 2017, BriaCell Therapeutics Corp. (TSXV: BCT) (BCTXF) announced that the U.S. FDA had granted clearance to initiate the Phase 1/2a clinical trial of BriaVax™ in patients with advanced breast cancer. This is an important step for the company and represents many years of hard work by management to get BriaVax back into the clinic, including finalizing the necessary CMC work around a new manufacturing process for the whole-cell vaccine.
I'm expecting the first patients to be dosed shortly. The principal investigator is Dr. Jarrod P. Holmes at St. Joseph Heritage Healthcare in Santa Rosa, California. Dr. Holmes is a Board Certified Oncologist and a leading expert in cancer vaccines. Cancer Insight, LLC, led by Dr. George Peoples, a surgical oncologist and leading expert in cancer vaccines, is managing the clinical study. Biologics Consulting is handling regulatory affairs.
The Phase 1/2a Program
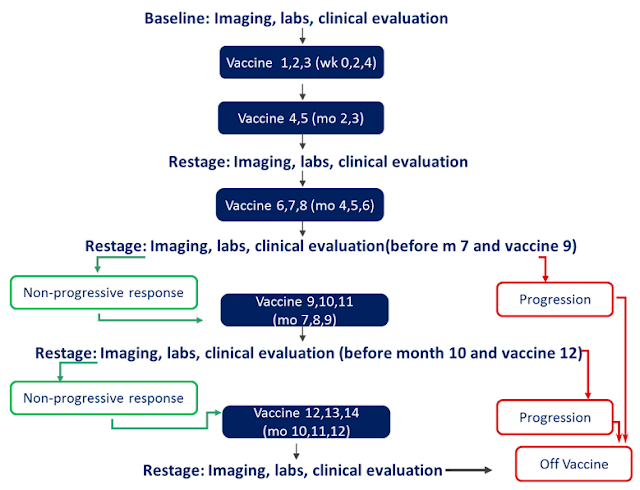
The Phase 1/2a trial (NCT03066947) is expected to enroll up to 24 late-stage cancer patients with recurrent and/or metastatic breast cancer who have failed at least one line of prior therapy (ECOG 0-2). The single-arm, open-label study is designed to determine the optimal dosing regimen and safety profile of the targeted immunotherapy. The primary endpoint is the incidence of treatment-emergent adverse events following multiple injections of BriaVax. The current protocol calls for inoculation of the vaccine at baseline and then every 2 weeks for one month (3 treatments), then monthly for up to one year.
Standard tumor assessments will be performed at baseline and then every 3 months. Important secondary outcome measures include overall survival (OS), objective response rate (ORR), progression free survival (PFS), and durability of tumor response. Other measures including patient quality of life, performance status, weight, and pain will also be measured. After at least 9 subjects have been treated safely, the dose of BriaVax may be escalated or decreased in subsequent patients based on the emerging data. Below is a schematic of the planned protocol:
CEO Steps Up To Fund The Trial
In a move not often seen by micro-cap biopharma companies, BriaCell President and CEO, Dr. William Williams, helped to fund the Phase 1/2a study with this own money. In late February 2017, Dr. Williams entered into a non-brokered private placement of approximately 5.42 million shares of BriaCell common stock at C24¢ per share. Proceeds of approximately C$1.5 million will be used to fund the Phase 1/2a study as well as develop a companion diagnostic platform known as BriaDx. At the time of the closing, Dr. Williams noted that his financial investment, "Reflects my confidence in the long-term value of the company."
Listen to Dr. Williams interview on UpTickNewswire >> LINK
How BriaVax Works
BriaVax is a proprietary allogeneic whole tumor cell vaccine that works as a targeted immunotherapy to stimulate the immune system. The recently initiated Phase 1/2a study noted above is a monotherapy program; however, management believes that BriaVax may by synergistic with currently approved checkpoint inhibitors such as Opdivo® and Keytruda®. In fact, the company is already working to add a roll-over protocol for patients that do not respond to BriaVax monotherapy where the combination with a checkpoint inhibitor is explored.
BriaVax expresses immune-stimulatory factors including HLA class I and II components. The cells overexpress multiple tumor-associated antigens including HER2 and PRAME. In addition to stimulating anti-tumor immunity, management observed an inrease in serum levels of soluble CD40 Ligand in the one patient who experienced significant tumor regression in the prior Phase 1 study compared to no increase in the patient who did not respond with tumor shrinkage. CD40L is a costimulatory protein found on antigen presenting cells, such as T cell, B cell, and natural killer (NK) cells that is required for their activation. Activation of CD40L has a variety of downstream effects, including dendritic cell maturation and an increase in serum levels of CD4+, CD8+, and NK cells known for their anti-tumor activities. BriaVax, serum CD40L might have prognostic potential.
BriaVax has also been genetically engineered to release sargramostim (granulocyte macrophage - colony-stimulating factor [GM-CSF]) for up-regulation of professional antigen-presenting cells. GM-CSF has been shown to be a potent immunostimulatory secreted molecule which induces tumor immunity and is believed to provide an antitumor effect that prolongs survival and disease-free survival. Also, part of the treatment regimen is the addition of low-dose cyclophosphamide (CY) prior to inoculation to down-regulate the activity of regulatory T cells and the use of interferon (IFN) alpha following inoculation to boost differentiation of dendritic cells.
Management believes that BriaVax should synergise well with other immunotherapies, including PD-1 inhibitors and CTLA4 inhibitors that eliminate immunosuppression. Immunostimulatory antibodies to molecules such as GITR and OX40 should also enhance responses to BriaVax. Investors have read before my use of the "gas and break" analogy for the BriaVax treatment regimen. Molecules like CY and checkpoint inhibitors like Opdivo and Keytruda take the "foot off the brake" with respect to T cell response and molecules like IFN-alpha and GITR and OX40 inhibitors "step on the gas" and evoke prolonged immune response.
The Role of BriaDx
BriaCell believes that they have identified a gene signature predictive of response to BriaVax. For example, following the successful completion of the second Phase 1 study (n=4), investigators observed potentially prolonged overall survival among three of the four patients (median OS: ~35 months); in addition, one patient, with an OS of 33.7 months, demonstrated clinically significant (>90%) tumor) regression.
Focusing more closely on these patients, BriaCell conducted a molecular analysis of both the BriaVax cell line and blood cells obtained from patients in the Phase 1 study. This "gene signature" analysis informed the company about a putative BriaVax mechanism of action and paved the way for the development of a potential companion diagnostic for both patient selection as well as monitoring during human clinical trials. For example, the one patients (subject A002) noted above who demonstrated clinically significant tumor regression shared both MHC class I (HLA-A) and class II (HLA-DRB3) alleles with BriaVax.

The basic findings, which were presented at AACR in April 2016 (Poster #2369), show that BriaVax expresses several genes known to encode tumor-associated antigens, such as HER2 and PRAME noted above. This type of direct antigen presentation combined with immune stimulatory factors including HLA class I and II components are hypothesized to result in activation of tumor-specific T cells. PRAME is expressed in 88% of primary melanomas and is a marker of poor prognosis in breast cancer. Other human malignancies that express PRAME include acute and chronic leukemias, medulloblastoma, lung cancer, head and neck cancer, renal carcinoma, and multiple myeloma.
Based on analysis of BriaVax specific alleles and HLA matching frequencies for various ethnic groups, management believes that 60% of all breast cancer patients will match at least one allele, with 20% matching both alleles. Recall, the uber-responder noted above matched both alleles and achieved near-complete remission. The company is also looking at ways to manufacture different cell lines of BriaVax that express other HLA types.
BriaCell Massively Undervalued
According to epidemiology data published in the Journal of the National Cancer Institute in 2013, approximately 80% of estimated 2.8 million breast cancer patients in the U.S. each year present with invasive disease. That equates to approximately 2.2 million cases. Roughly one-quarter of these will metastasize and 20% will fail first-line therapy and be eligible for treatment with a therapeutic candidate like BriaVax. That equates to approximately 100,000 patients per year.
If we conservatively assume that only the 20% that match both BriaVax alleles receive the drug (~20,000 patients) and that management can capture 25% market share, the likely peak penetration for BriaVax is 5,000 patients under the most conservative base case. Priced at $48,000 per course of treatment (8 vaccines over 6 months), the estimated peak sales of BriaVax is $250 million. A more aggressive assumption that 60% of the patients that match at least one HLA allele may try BriaVax expands the peak sales number to $1 billion.
The company is also looking at the potential to use BriaVax in combination with other treatment options, such as checkpoint inhibitors, looking for an additive or synergistic effect. This is a logical path for BriaCell because checkpoint inhibitors (such as PD-1, PD-L1, CTLA4) eliminate immunosuppression that should improve the efficacy of BriaVax. The combination with immunostimulatory antibodies (GITR, OX40) should also enhance response to BriaVax - recall my "gas and break" analogy.
Improved response may move BriaVax from second-line to first-line therapy. This is where the numbers start to get really large because the first-line market is 4X the size of the second-line market. Peak sales of BriaVax could be $1 billion (conservative HLA matching criteria) to $4 billion (more liberal HLA matching criteria). First-line patients may also live longer than second-line patients, potentially expanding the number of BriaVax inoculations beyond the 8 vaccines over 6 months I noted above.
I think BriaVax is incredibly intriguing and with a current market capitalization (USD) of only $24 million, BriaCell looks like a very interesting "lotto play" given my belief that BriaVax peak sales ranges somewhere between $250 million (conservative) to $4 billion (aggressive). Even with the most conservative valuation assumptions, the shares look reasonably cheap!
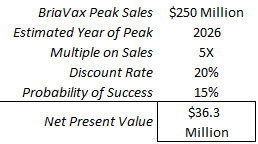
I think the shares have 50% upside even when applying a relatively low probability of success. Positive Phase 1/2a data as a monotherapy and confirmation that BriaVax synergizes well with checkpoint inhibitors increase my peak sales and my probability of success inputs. By the end of the year when we see initial data from this Phase 1/2a study, my model could easily peg BriaVax valuation at over $100 million. This would be a 4X return from today.
Conclusion
BriaCell Therapeutics remains one of my favorite under-the-radar immuno-oncology names. BriaVax is an allogeneic whole cell vaccine, and thus not hampered by the immune masking or the logistical commercial nightmares of previous autologous approaches like Dendreon's Provenge®. Instead, BriaVax seems to offer the ideal immunotherapy - powerful enough to induce both a broad-scale innate and adaptive immune reaction, targeted to reduce systemic side-effects, and personalized based on genetic biomarkers to improve the odds of success. There is also a strong scientific rationale for a combination of BriaVax with checkpoint inhibitors and expansion of the program into additional solid tumors or hematologic malignancies. Finally, the CEO just invested $1.5 million of his own money into the story and that alone should warrant investors attention.
Disclosure: Please see important information about BioNap, Inc. and our relationship with names in this article in our more


