
JPM: Covid Scenarios For 2021
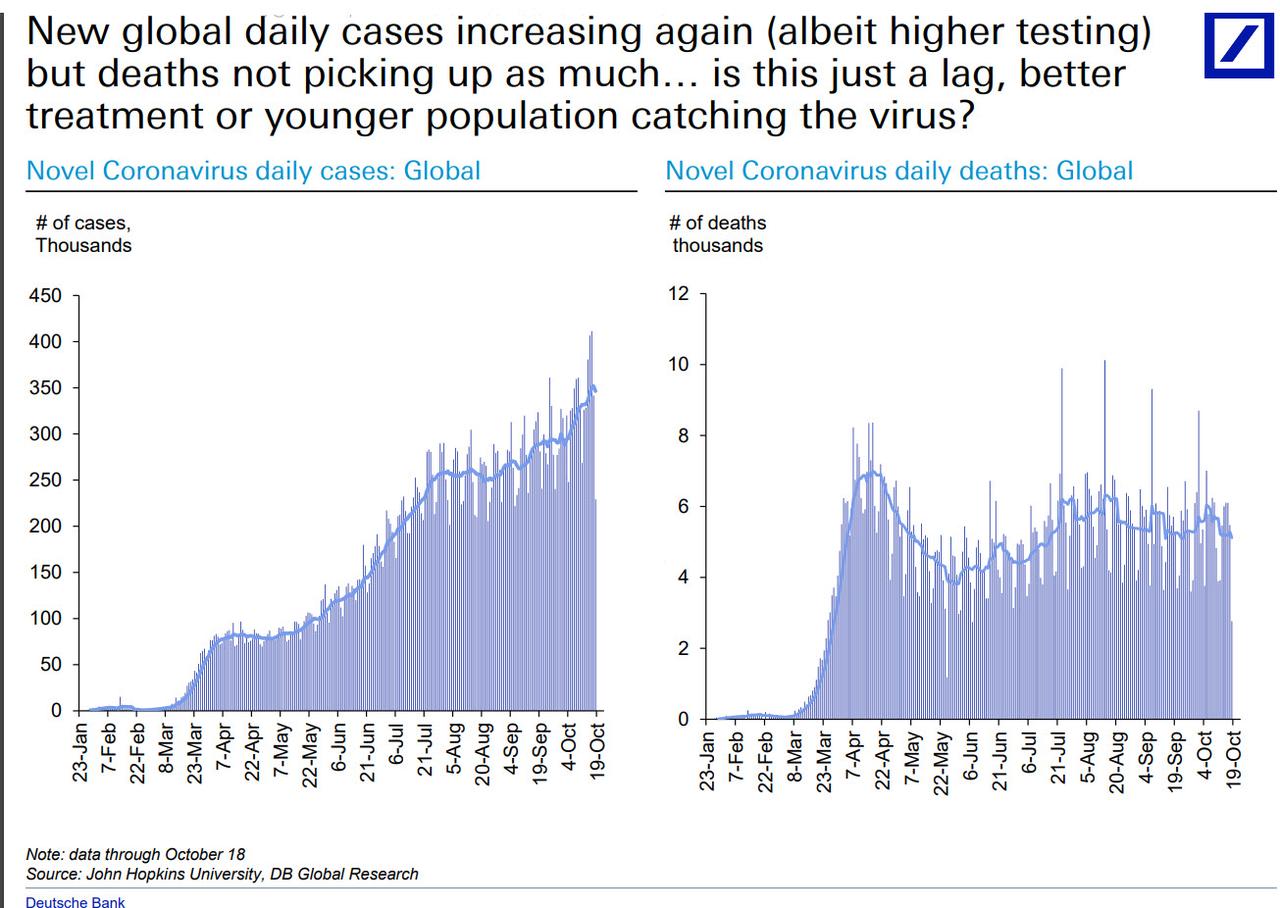
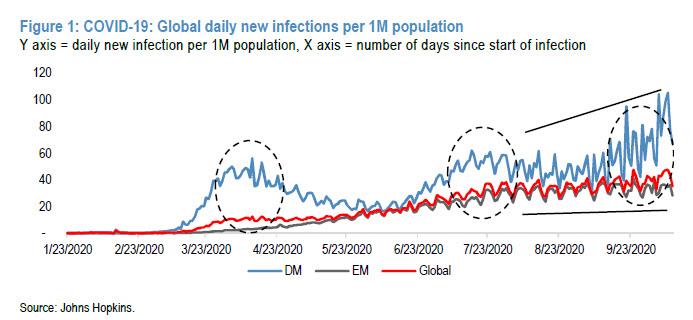
COVID resurgence risks are flashing, as new infection cases rose 4% W/W, to a record ~350k per day (vs. 228k/254k/283k in Jul/Aug/Sep) largely due to record test numbers, yet this is more than offset by a diminished and stubbornly low mortality rate (2.8% vs. peak: 7.2%), which may be due to better treatment as well as a younger population catching the virus, further mitigated by vaccine/treatment progress...
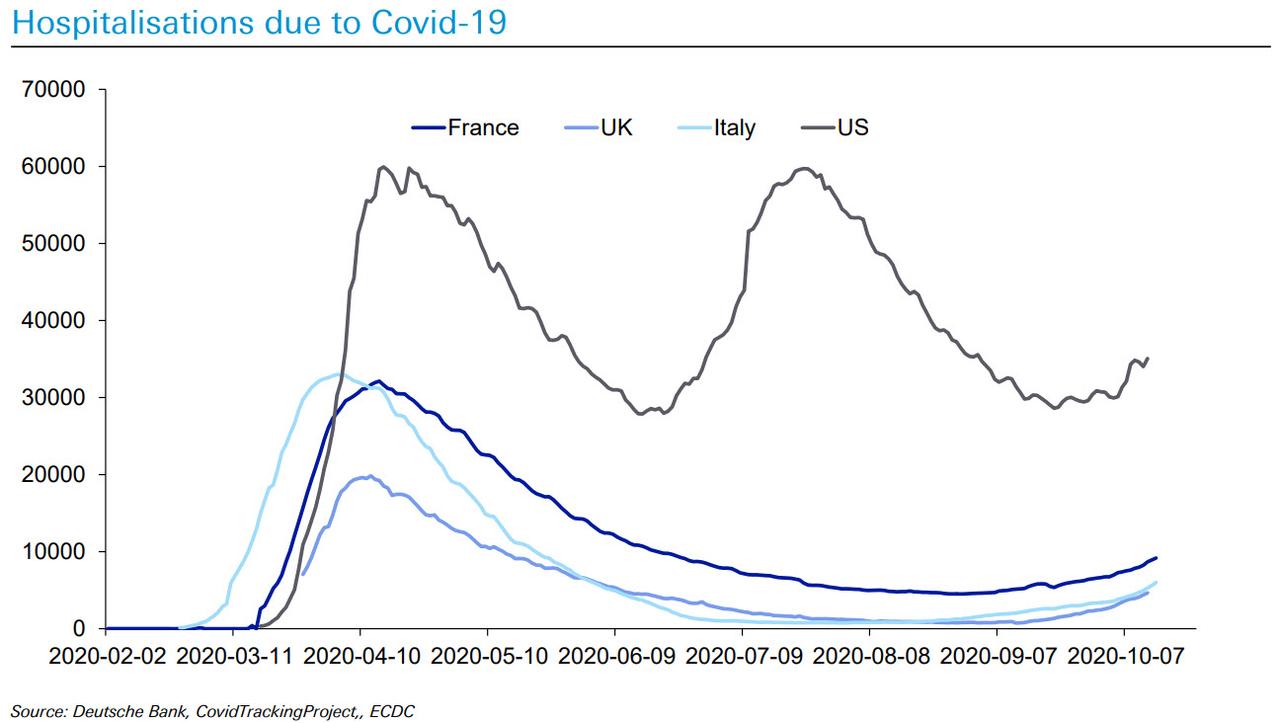
... while hospitalizations due to COVID remain very much under control...
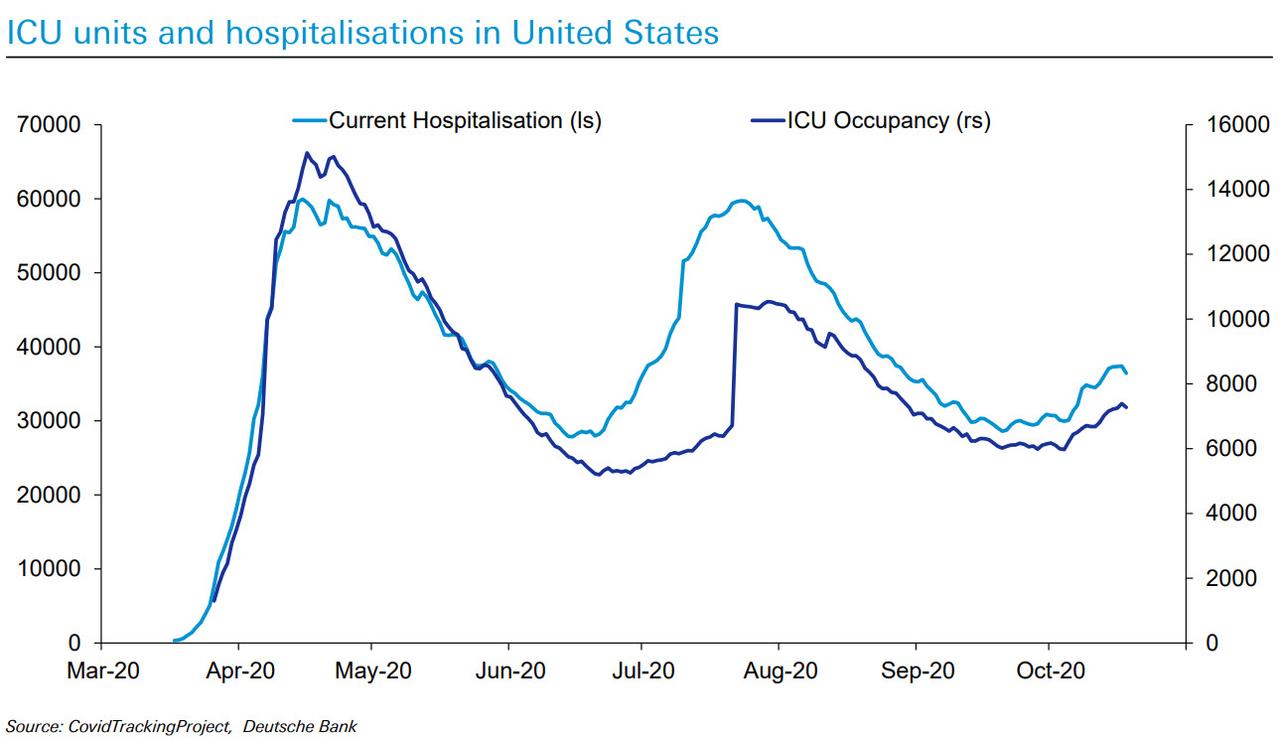
... and ICU units in the US were less full during the second wave, even as patients in hospital were similar. While the curve is again starting to edge up, it's not to critical levels.
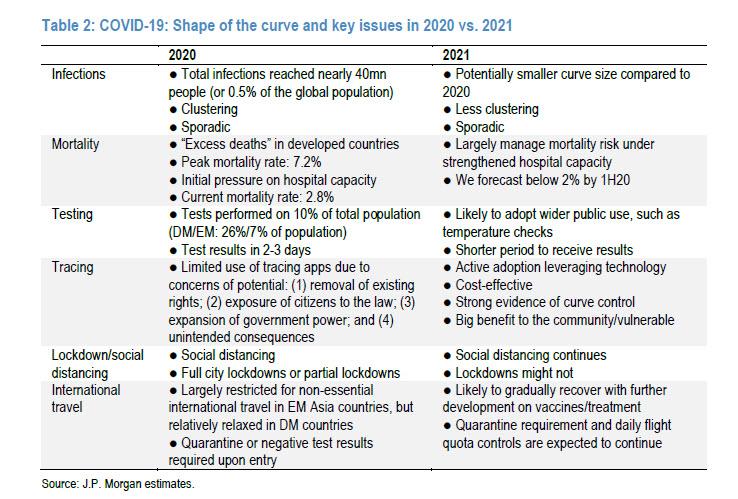
In an attempt to reconcile the curve’s persisting beyond year-end, JPMorgan's MW Kim presents several potential 2021 scenarios. Noting further progress in vaccine/treatment, the strategist highlights:
- the mortality rate could decline below 2% by 1H21E;
- infections could be less clustered, sporadic and perhaps smaller-scale in third/fourth waves;
- lockdowns may decline as a primary response in 2021 due to their economic burden, rising public stress on social distancing, and fiscal budget limitations.
Additionally, due to the improvement in treatment and growing social preparedness, JPM argues that public health strategy should shift from “infection control” to "patient treatment."
With that in mind, here are the top ways in which the response to COVID in 2021 will differ markedly from 2020, according to JPMorgan.
Public Health Strategy: 2020 will not be 2021
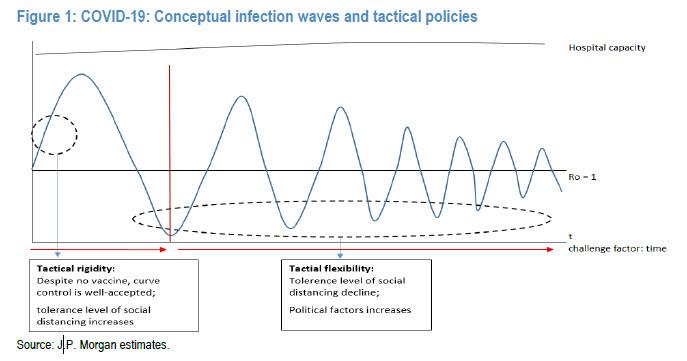
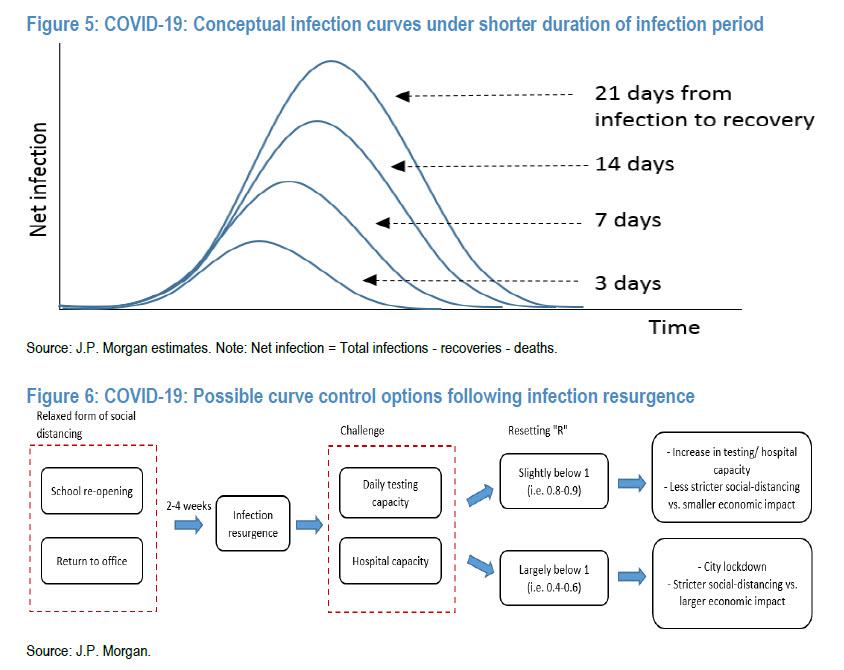
The primary public health strategy in 2020 has been to suppress the infection curve, as the initial reported mortality rate was very high (peak of 7.2% in late April). Thus, reducing human-to-human contacts (or pulling back the secondary infection rate, “R0”) via stricter social distancing and/or lockdown has worked to reduce infections and thus to control the mortality risk YTD, in JPM's view. However, this approach proved to be costly, with a greater burden on the economy and rising social stress from tolerating the social distancing. Also, following hospital capacity strengthening and better medical treatment, the mortality rate is under far better control. Besides more realistic target R resetting close to 1, the public health focus is to shift toward “patient treatment,” as society has accumulated more knowledge/experience with COVID-19 (i.e., less uncertainty or unknown risk).
Looking ahead, JPMorgan suggests dour things in next year’s public health strategy:
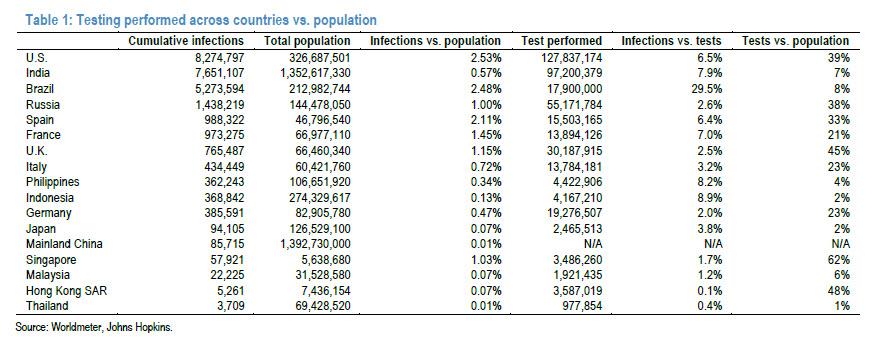
- First, testing should be free or largely subsidized by government to encourage large-scale testing of susceptible groups. The asymptomatic carriers of COVID-19 can still transmit the disease to a similar degree as symptomatic patients. According to a study in The Lancet, in early April, Belgium’s ministry of health implemented a mass testing campaign in long-term care facilities. 8,343 people tested positive among the 280,427 people who were tested (3%). 6,244 of the positive cases (75%) were asymptomatic. Similar viral loads have been reported between symptomatic and asymptomatic cases, making the transmission and spread of the virus possible for both groups. Thus, extensive testing is the key method for identifying asymptomatic cases at an early stage and controlling virus transmission.
- Second, potential drug candidates should be fully included under public/private insurance coverage. As more treatments are being developed for COVID-19, it could be possible for government to extend treatment services under insurance coverage. One potential complication is that as many COVID-19-related potential drugs are still awaiting approval, existing insurance coverage plans seem to not fully cover detailed drugs for treatment. This could be protocol to be amended once efficacy is partially confirmed in certain groups of infection populations (i.e., milder symptom groups, asymptomatic groups, etc.) to shorten the recovery period and, thus, reduce the infection curve/scale. According to WHO, out-of-pocket payments may create a financial barrier to accessing health services. Co-payments do not selectively deter “unnecessary” use, but reduce the use of all health services, particularly among people with chronic conditions and poorer people. Therefore, with co-payments in place, people may delay seeking treatment or be prevented from obtaining health services, which would make it more difficult to control outbreaks
- and put more people at risk. Indicatively, at this stage, China has fully removed treatment expenses for COVID-19. Ireland has removed user charges for remote primary care consultations with people who may have COVID-19. Belgium has initiated teleconsultations in primary care and removed user charges for this new method. France has simplified administrative requirements for people with chronic conditions benefiting from co-payment exemptions. Estonia has drawn on private facilities to increase access to testing that is free from co-payments.
- Third, the current infection control strategy of temporarily closing hospitals, workplaces and schools following infection reporting should be amended in a way that does not involve closing. Currently, public places are closed following infection case reporting to test all available susceptible people. When infections have large clusters, this approach can be helpful in interrupting the transmission rate. However, as observed in the second/third waves in Korea and HK SAR, infections become sporadic with smaller clusters. Thus, the current manual on infection control could lead to large economic/social burden if the infection curve repeats in 2021 with more random outbreaks, as current testing needs two to three days to generate results. Furthermore, as even JPMorgan admits, by far, the overall mortality risk of the working population and young age group looks reasonably low, and it is hard to identify all asymptomatic cases. As a certain level of social distancing is to continue in 2021, keeping public activities open might be a better risk-reward decision according to JPM. Additionally, JPM expects new methods of low-cost and rapid testing to be developed and utilized in public places in the next year. Potential developments in rapid testing with results out in less than five minutes and widely used in workplaces, schools, etc., is a well-expected scenario. These efforts could reduce overall infection risk levels in public places and, thus, overall infection risks in the community.
- Fourth, large-scale antibody testing (~1-5% of the total population) would allow a better understanding of a community’s immunity status. At this stage, the effective period of antibodies remains unclear, so we expect further research on antibodies, along with larger-scale antibody tests, to be carried out next year.
Picturing the curve in 2021
JPMorgan summarizes the key expected trends in the curve of infections below, and predicts that "overall risk levels of infection development and mortality should decline further after this winter." adding that it does not expect lockdowns to be a major public health strategy to interrupt the transmission rate in 2021. Test and tracing are expected to be efficient and could be better accepted by the public. That said, the largest US bank remains cautious on full-scale international travel even beyond 2020.
Infections: 40mn YTD, recovery: 70%
JPMorgan expects a series of infection waves potentially globally/in Asia until a vaccine is available to large populations. Contrary to earlier concerns, the second-wave infection scale and mortality risk appear more controlled across Asian countries compared to DM countries. This could be driven by limited human mobility YTD, flexible public policy resetting target R below 1 with sustainable social distancing and strong controls leveraging technology in EM Asian countries. That said, the shape of the global infection curve could be milder and smaller after this winter due to developments in treatment (faster recovery), smaller susceptibility under rising public awareness, and faster public responses on secondary infection rate (R0) control.
Mortality: 2.8% (vs. peak: 7.2%)
JPMorgan believes that the mortality rate (= death/infections) could decline below 2% by the end of 1H21 (vs. current: 2.8%), if current developments continue. More importantly, the bank does not expect “excess deaths” in 2021, as was observed in developed countries this year. COVID-19 has led to a small impact on Asian countries’ annual mortality rates. Reported deaths due to COVID-19 are only 0.01-0.18% of annual deaths in Asian countries. According to Euro MOMO data, 17 of the 24 countries in Europe have shown improving mortality rates following the spike in early April.

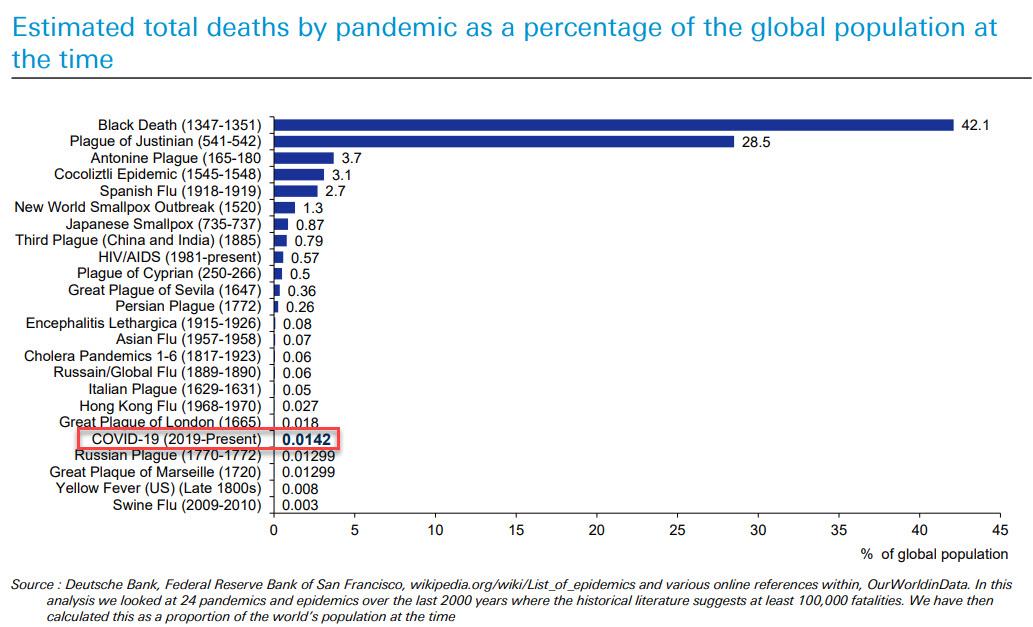
Incidentally, here is a chart putting the death toll of COVID in the context of the world's top-20 pandemics:
Curve control
Beyond 2020, JPMorgan does not expect partial/full lockdowns to be a key public health strategy. Managing R0 around 1 (R0 ≤1) under reasonable social distancing levels and medical treatments to shorten the recovery period could be more in focus. Medical treatments could be another strong way to control the curve, as the secondary infection rate would be simplified as a function of transmission rate and the recovery rate among the susceptible. If the average recovery period were to shorten from about two weeks currently to less than one week, this would open a new window for curve control, the economy and the public stress level on social distancing.
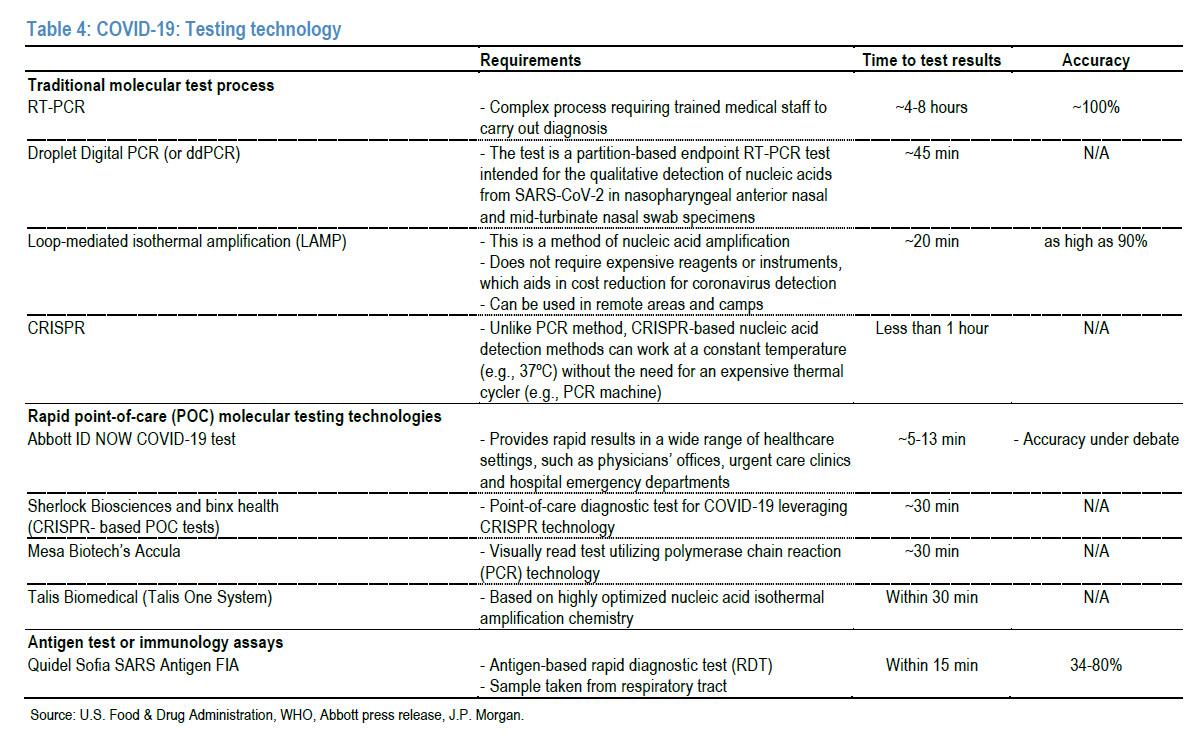
Testing
Schools and offices are expected to remain open in 2021. Regular testing is to be largely implemented, as test results could be checked in a short period. The most common COVID-19 testing is laboratory-based RT-PCR, which takes about four to eight hours for results to be delivered. Although accuracy is as high as 100%, this technique requires specialist kits, trained professionals and time. Also, testing is limited to certified laboratories only. In addition to traditional laboratory testing methods such as RT-PCR, dd PCR and loop mediated isothermal amplification (LAMP), several other rapid point-of-care (POC) testing technologies have been used to detect SARS-CoV-2 (see Table below). These fast-testing technologies detect the presence of SARS-CoV-2 in 5-30 minutes. However, WHO recommends traditional molecular testing methods (e.g., RT-PCR) for the identification and laboratory confirmation of COVID-19 cases. In order to return to work/school, testing daily or weekly for all groups prior to entering a public place could be essential. At this stage, this ideal process, similar to a daily temperature check, is not possible, as tests cost ~US$20-40 each and take 15-30 minutes at best to get results, and test accuracy may not be 100%.
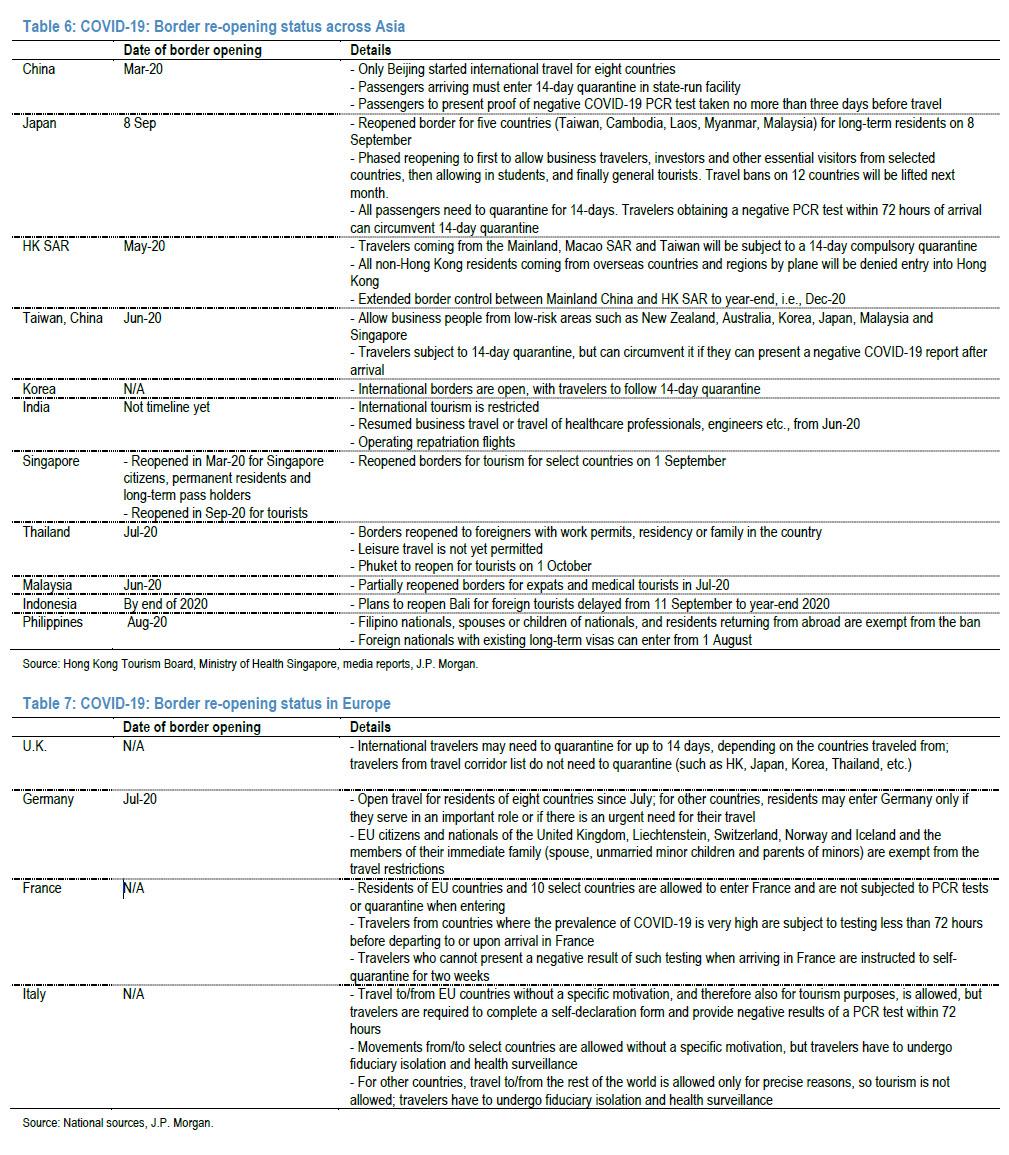
Border control
Borders are expected to gradually re-open, according to JPM, even as quarantine requirements (7-14 days) and daily flight quota controls for testing at arrival continue in 2021. Some countries have launched “travel bubbles,” which are partnerships between nearby countries that have demonstrated considerable success in containing COVID-19 within their respective borders. These countries re-establish connections by opening up borders to one another and allowing people to travel freely within the zone without undergoing on-arrival quarantine. On 15 October, Singapore and Hong Kong said they had reached a preliminary agreement to establish a travel bubble, allowing travelers of all kinds to bypass quarantine.
To summarize, this is how JPM pictures COVID in 2021:
Infections: expect a series of waves rippling globally/in Asia. The infection curve could be milder and smaller after winter passes,
- factoring in a faster recovery, smaller susceptibility and a faster public response.
- Mortality: The bank expects a mortality rate (= death/infections) decline below 2% by end-1H21 (vs. current: 2.8%).
- Curve control: JPM does not foresee lockdowns as a key public health strategy beyond 2020. Managing R0 ≤1, rather than full suppression, could become a primary focus.
- Testing: Schools and offices are expected to remain open in 2021. Regular testing is likely to be widely implemented as test results become available faster (link).
- Border control: While borders will gradually re-opening, quarantines (7-14 days) and daily flight quota controls at airports will continue in 2021.
Disclaimer: Copyright ©2009-2020 ZeroHedge.com/ABC Media, LTD; All Rights Reserved. Zero Hedge is intended for Mature Audiences. Familiarize yourself with our legal and use policies every ...
more

